

Maintaining the permanence principle for death during in situ normothermic regional perfusion for donation after circulatory death organ recovery: A United Kingdom and Canadian proposal
- PMID: 31922653
- PMCID: PMC7540256
- DOI: 10.1111/ajt.15775
Maintaining the permanence principle for death during in situ normothermic regional perfusion for donation after circulatory death organ recovery: A United Kingdom and Canadian proposal
Abstract
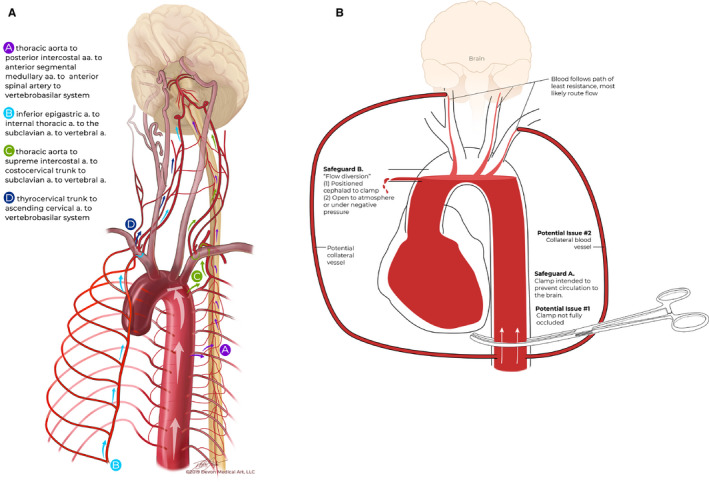
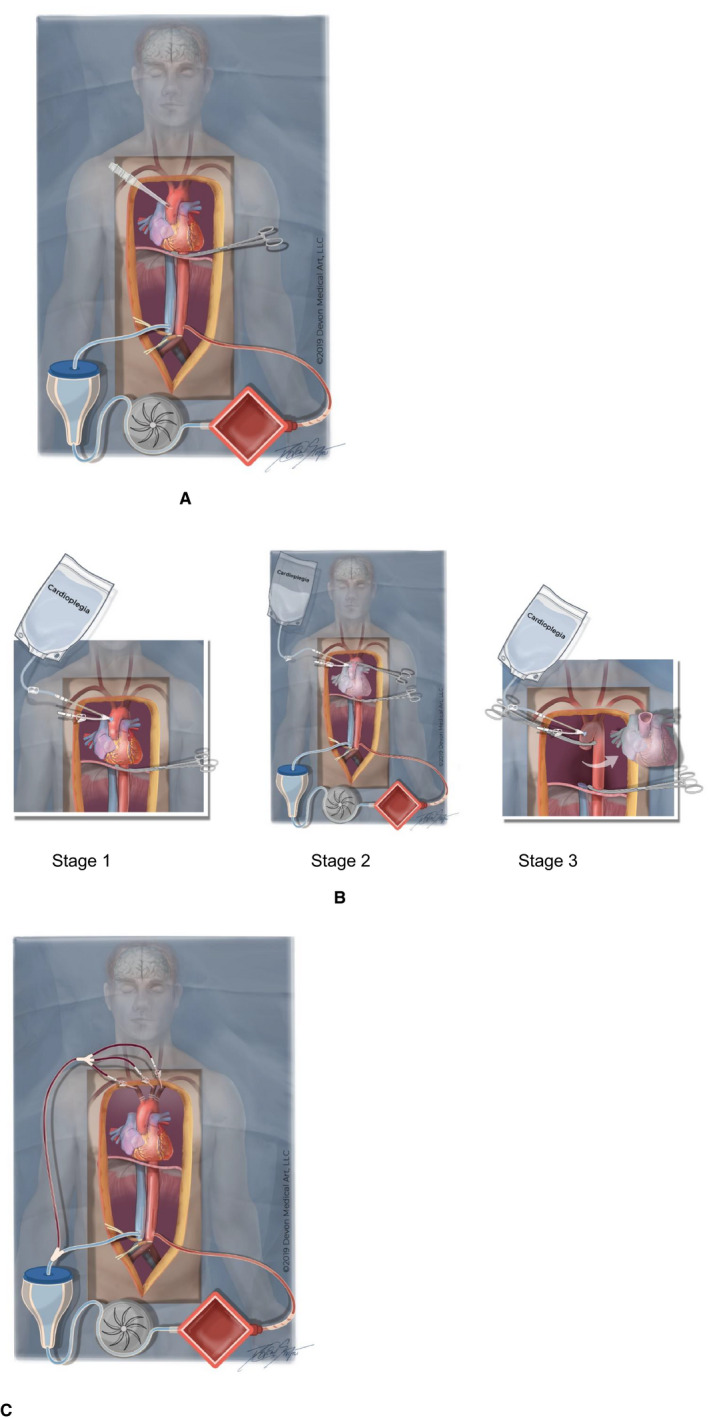
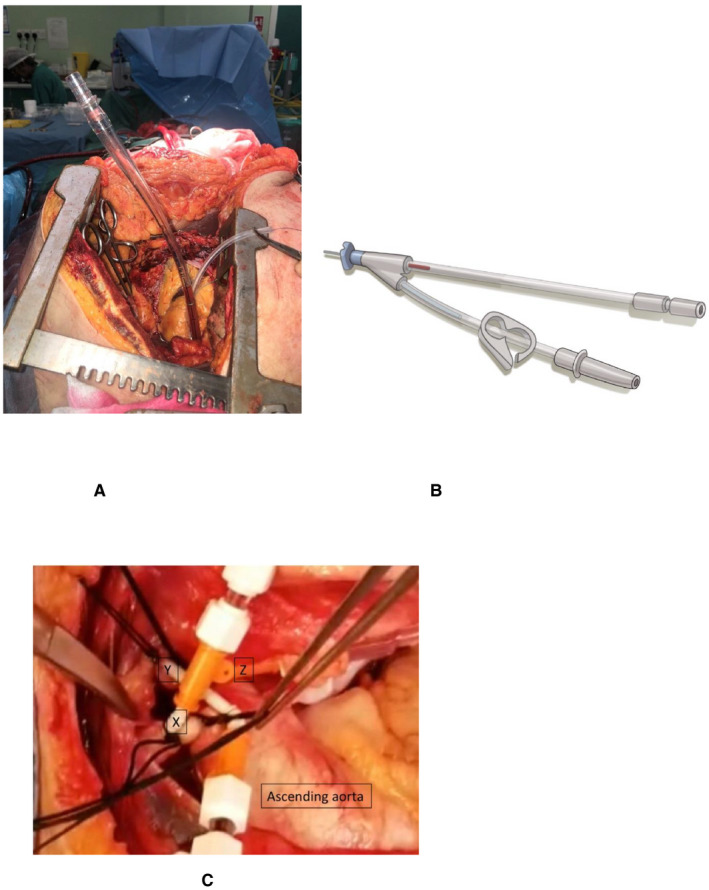
There is international variability in the determination of death. Death in donation after circulatory death (DCD) can be defined by the permanent cessation of brain circulation. Post-mortem interventions that restore brain perfusion should be prohibited as they invalidate the diagnosis of death. Retrieval teams should develop protocols that ensure the continued absence of brain perfusion during DCD organ recovery. In situ normothermic regional perfusion (NRP) or restarting the heart in the donor's body may interrupt the permanent cessation of brain perfusion because, theoretically, collateral circulations may restore it. We propose refinements to current protocols to monitor and exclude brain reperfusion during in situ NRP. In abdominal NRP, complete occlusion of the descending aorta prevents brain perfusion in most cases. Inserting a cannula in the ascending aorta identifies inadequate occlusion of the descending aorta or any collateral flow and diverts flow away from the brain. In thoracoabdominal NRP opening the aortic arch vessels to atmosphere allows collateral flow to be diverted away from the brain, maintaining the permanence standard for death and respecting the dead donor rule. We propose that these hypotheses are correct when using techniques that simultaneously occlude the descending aorta and open the aortic arch vessels to atmosphere.
Keywords: donors and donation: donation after circulatory death (DCD); editorial/personal viewpoint; ethics; extracorporeal membrane oxygenation (ECMO); organ perfusion and preservation; organ procurement; organ procurement and allocation.
© 2020 The Authors. American Journal of Transplantation published by Wiley Periodicals, Inc. on behalf of The American Society of Transplantation and the American Society of Transplant Surgeons.
Conflict of interest statement
The authors of this manuscript have conflicts of interest to disclose as described by the
Figures
References
-
- Canadian Organ Replacement Register . e‐Statistics On Organ Transplants, Waiting Lists And Donors. https://www.cihi.ca/en/e-statistics-on-organ-transplants-waiting-lists-a.... Published 2018. Accessed September 3, 2019.
-
- NHS Blood and Transplant . Organ Donation and Transplantation Activity Report 2017/18. https://nhsbtdbe.blob.core.windows.net/umbraco-assets-corp/12300/transpl.... Published 2018. Accessed September 3, 2019.
-
- Detry O, Van Deynse D, Van Vlierberghe H, Pirenne J. Organ procurement and transplantation in Belgium. Transplantation. 2017;101(9):1953‐1955. - PubMed
-
- Leiden H, Haase‐Kromwijk B, Hoitsma A, Jansen N. Controlled donation after circulatory death in the Netherlands: more organs, more efforts. The Netherlands Journal of Medicine. 2016;74(7):285‐291. - PubMed
-
- Manara AR, Murphy PG, Ocallaghan G. Donation after circulatory death. Br J Anaesth. 2012;108(Suppl 1):i108‐i121. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
