

20-year follow-up study of physical morbidity and mortality in relationship to antipsychotic treatment in a nationwide cohort of 62,250 patients with schizophrenia (FIN20)
- PMID: 31922669
- PMCID: PMC6953552
- DOI: 10.1002/wps.20699
20-year follow-up study of physical morbidity and mortality in relationship to antipsychotic treatment in a nationwide cohort of 62,250 patients with schizophrenia (FIN20)
Abstract
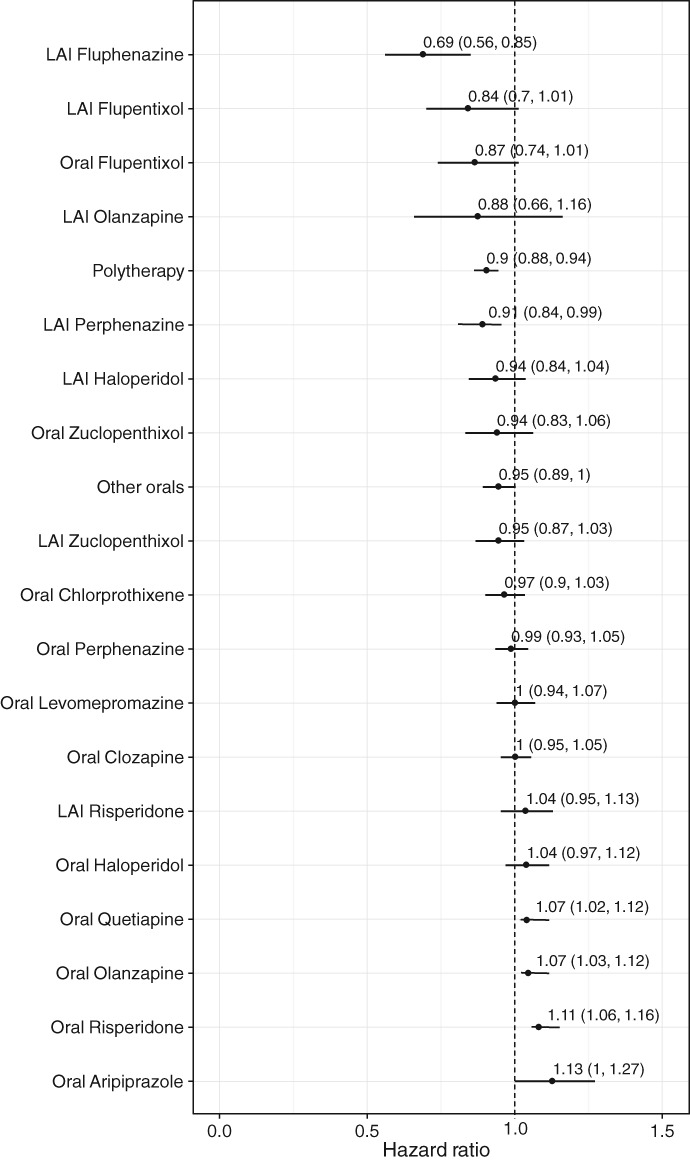
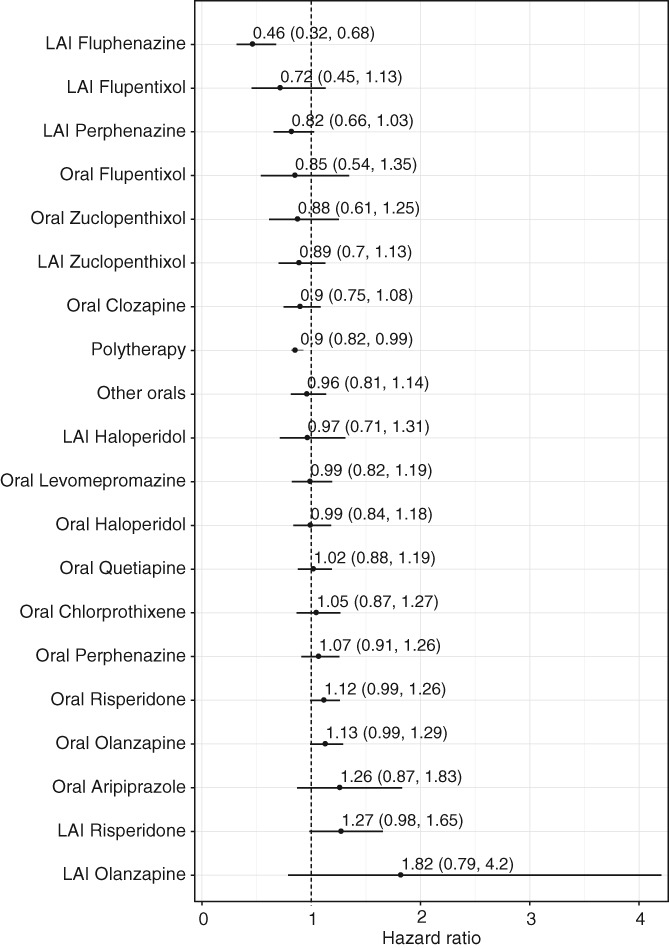
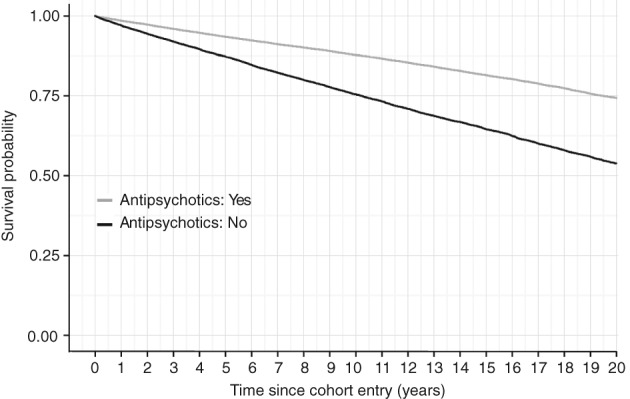
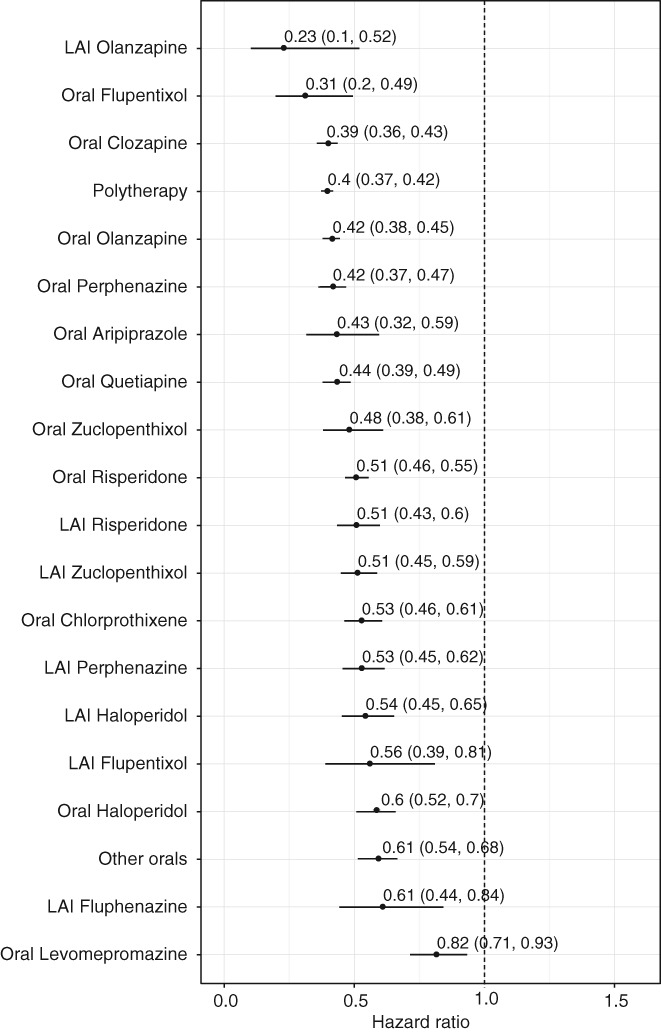
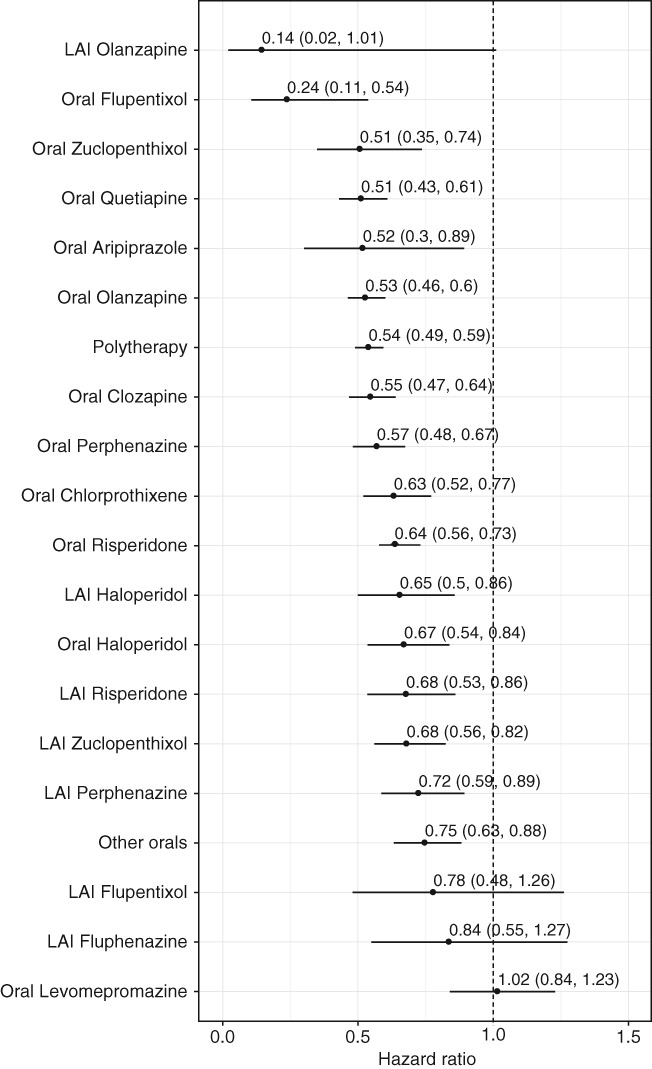
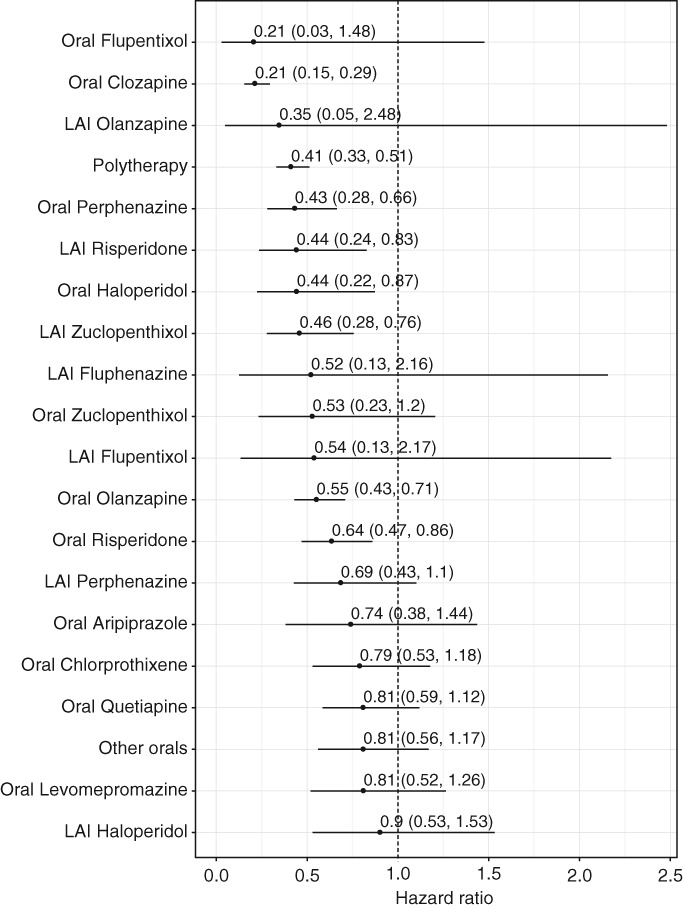
Antipsychotics are effective in preventing relapses of schizophrenia, but it is generally believed that their long-term use is harmful for patients' physical well-being. However, there are no long-term studies which have verified this view. This nationwide, register-based cohort study aimed to assess the risk of hospitalization due to physical health problems, as a marker for severe physical morbidity, and the risk of all-cause mortality, as well as of cardiovascular and suicidal death, associated with antipsychotic use in all patients treated for schizophrenia in inpatient care between 1972 and 2014 in Finland (N=62,250), with up to 20 years of follow-up (median: 14.1 years). The use of antipsychotic drugs (i.e., use of any antipsychotic compared with non-use) and the use of specific antipsychotics were investigated, and outcomes were somatic and cardiovascular hospitalization, and all-cause, cardiovascular and suicide death. Hospitalization-based outcomes were analyzed by a within-individual design to eliminate selection bias, comparing use and non-use periods in the same individual by stratified Cox model. Mortality outcomes were assessed by traditional between-individual Cox multivariate models. The adjusted hazard ratios (aHRs) for any somatic hospitalization and cardiovascular hospitalization were 1.00 (95% CI: 0.98-1.03) and 1.00 (95% CI: 0.92-1.07) during use of any antipsychotic compared to non-exposure periods within the same individual. The aHRs were 0.48 (95% CI: 0.46-0.51) for all-cause mortality, 0.62 (95% CI: 0.57-0.67) for cardiovascular mortality, and 0.52 (95% CI: 0.43-0.62) for suicide mortality during use vs. non-use of any antipsychotic. The most beneficial mortality outcome was associated with use of clozapine in terms of all-cause (aHR=0.39, 95% CI: 0.36-0.43), cardiovascular (aHR=0.55, 95% CI: 0.47-0.64) and suicide mortality (aHR=0.21, 95% CI: 0.15-0.29). The cumulative mortality rates during maximum follow-up of 20 years were 46.2% for no antipsychotic use, 25.7% for any antipsychotic use, and 15.6% for clozapine use. These data suggest that long-term antipsychotic use does not increase severe physical morbidity leading to hospitalization, and is associated with substantially decreased mortality, especially among patients treated with clozapine.
Keywords: Schizophrenia; all-cause mortality; antipsychotic treatment; cardiovascular mortality; clozapine; hospitalization; physical morbidity; suicide.
© 2020 World Psychiatric Association.
Figures
References
-
- Leucht S, Tardy M, Komossa K et al. Antipsychotic drugs versus placebo for relapse prevention in schizophrenia: a systematic review and meta‐analysis. Lancet 2012;379:2063‐71. - PubMed
LinkOut - more resources
Full Text Sources
