

Cervical esophageal perforation caused by the use of bougie during laparoscopic sleeve gastrectomy: a case report and review of the literature
- PMID: 31924187
- PMCID: PMC6954567
- DOI: 10.1186/s12893-020-0679-1
Cervical esophageal perforation caused by the use of bougie during laparoscopic sleeve gastrectomy: a case report and review of the literature
Abstract
Background: Obesity is considered a chronic disease with an increasing prevalence worldwide during the last decades. Laparoscopic sleeve gastrectomy is the most commonly performed bariatric procedure, due to its relative safety and long-term efficacy. The use of bougie to ensure correct size of the gastric tube is part of the standard operation, usually placed by the anesthesiologist and with a very low rate of complications. We report the first case, to our knowledge, of a cervical esophageal perforation caused by the use of bougie during laparoscopic sleeve gastrectomy.
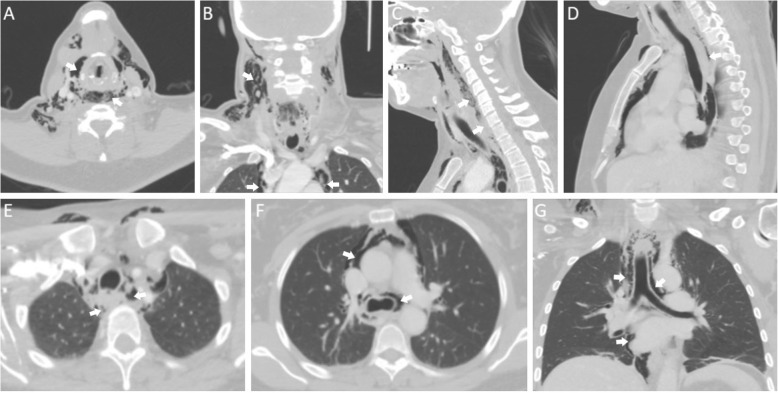
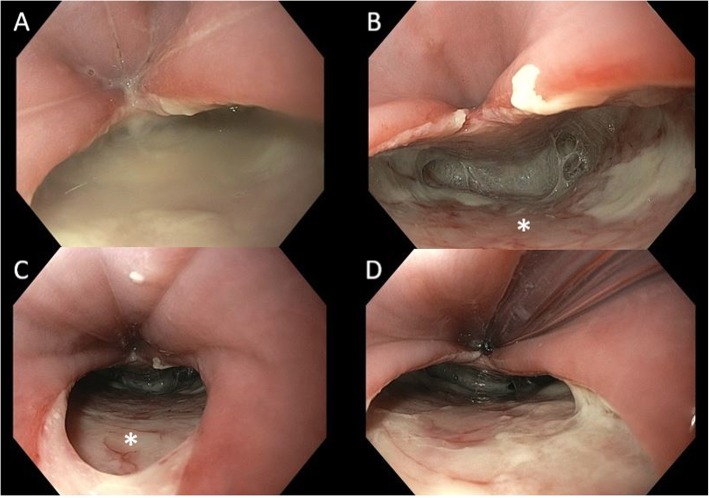
Case presentation: The complication occurred in a previously healthy 42-year old female patient who underwent laparoscopic sleeve gastrectomy for class 1 obesity (BMI 31 kg/m2) and was diagnosed the first post-operative day. She was subsequently treated with an emergency thoracoscopy and evacuation of a mediastinal fluid collection, with additional neck incision for primary closure of the esophageal defect which was reinforced with a sternocleidomastoid muscle flap. The post-operative course was uneventful.
Conclusions: We made a literature review to better understand the options considering the diagnosis and treatment in case of very proximal iatrogenic esophageal perforations. The risks related to the use of bougie during surgery should not be underestimated, and its insertion must be done with extreme caution. Esophageal perforation is still a challenging, life threatening complication where prompt diagnosis and adequate treatment are essential.
Keywords: Bougie; Case report; Esophageal perforation; Laparoscopic sleeve gastrectomy.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
