

Progression of the smoking epidemic in high-income regions and its effects on male-female survival differences: a cohort-by-age analysis of 17 countries
- PMID: 31924192
- PMCID: PMC6954612
- DOI: 10.1186/s12889-020-8148-4
Progression of the smoking epidemic in high-income regions and its effects on male-female survival differences: a cohort-by-age analysis of 17 countries
Abstract
Background: Of all lifestyle behaviours, smoking caused the most deaths in the last century. Because of the time lag between the act of smoking and dying from smoking, and because males generally take up smoking before females do, male and female smoking epidemiology often follows a typical double wave pattern dubbed the 'smoking epidemic'. How are male and female deaths from this epidemic differentially progressing in high-income regions on a cohort-by-age basis? How have they affected male-female survival differences?
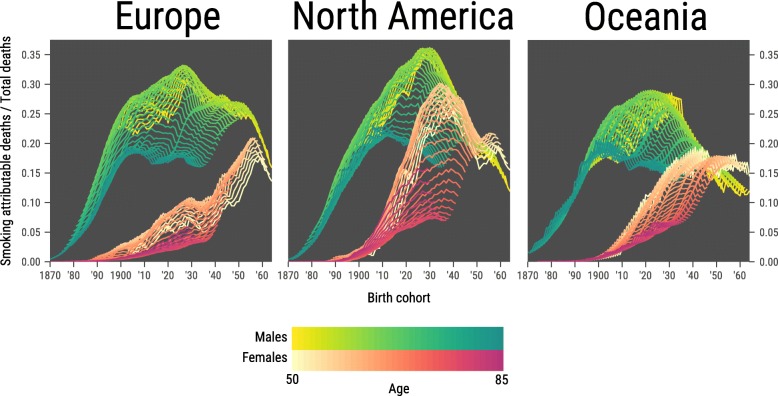
Methods: We used data for the period 1950-2015 from the WHO Mortality Database and the Human Mortality Database on three geographic regions that have progressed most into the smoking epidemic: high-income North America, high-income Europe and high-income Oceania. We examined changes in smoking-attributable mortality fractions as estimated by the Preston-Glei-Wilmoth method by age (ages 50-85) across birth cohorts 1870-1965. We used these to trace sex differences with and without smoking-attributable mortality in period life expectancy between ages 50 and 85.
Results: In all three high-income regions, smoking explained up to 50% of sex differences in period life expectancy between ages 50 and 85 over the study period. These sex differences have declined since at least 1980, driven by smoking-attributable mortality, which tended to decline in males and increase in females overall. Thus, there was a convergence between sexes across recent cohorts. While smoking-attributable mortality was still increasing for older female cohorts, it was declining for females in the more recent cohorts in the US and Europe, as well as for males in all three regions.
Conclusions: The smoking epidemic contributed substantially to the male-female survival gap and to the recent narrowing of that gap in high-income North America, high-income Europe and high-income Oceania. The precipitous decline in smoking-attributable mortality in recent cohorts bodes somewhat hopeful. Yet, smoking-attributable mortality remains high, and therefore cause for concern.
Keywords: Health inequality; Life expectancy; Mortality; Sex differences; Smoking epidemic.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


Similar articles
-
Changing contribution of smoking to the sex differences in life expectancy in Europe, 1950-2014.Eur J Epidemiol. 2020 Sep;35(9):835-841. doi: 10.1007/s10654-020-00602-x. Epub 2020 Jan 22. Eur J Epidemiol. 2020. PMID: 31970573 Free PMC article.
-
The Role of Smoking in Country Differences in Life Expectancy Across Europe, 1985-2014.Nicotine Tob Res. 2021 Jan 7;23(1):152-160. doi: 10.1093/ntr/ntaa011. Nicotine Tob Res. 2021. PMID: 31943074 Free PMC article.
-
Understanding longevity in Hong Kong: a comparative study with long-living, high-income countries.Lancet Public Health. 2021 Dec;6(12):e919-e931. doi: 10.1016/S2468-2667(21)00208-5. Epub 2021 Nov 10. Lancet Public Health. 2021. PMID: 34774201
-
Health at advanced age: social inequality and other factors potentially impacting longevity in nine high-income countries.Maturitas. 2013 Feb;74(2):137-47. doi: 10.1016/j.maturitas.2012.11.013. Epub 2012 Dec 28. Maturitas. 2013. PMID: 23276601 Review.
-
The Australian mortality decline: all-cause mortality 1788-1990.Aust N Z J Public Health. 1998 Feb;22(1):27-36. doi: 10.1111/j.1467-842x.1998.tb01141.x. Aust N Z J Public Health. 1998. PMID: 9599849 Review.
Cited by
-
Estimation of smoking-related mortality and its contribution to educational inequalities in life expectancy in Spain: an observational study, 2016-2019.BMJ Open. 2022 Aug 10;12(8):e059370. doi: 10.1136/bmjopen-2021-059370. BMJ Open. 2022. PMID: 35948385 Free PMC article.
-
Smoking and inequalities in mortality in 11 European countries: a birth cohort analysis.Popul Health Metr. 2021 Jan 30;19(1):3. doi: 10.1186/s12963-021-00247-2. Popul Health Metr. 2021. PMID: 33516235 Free PMC article.
-
Biomarkers of aging: from molecules and surrogates to physiology and function.Physiol Rev. 2025 Jul 1;105(3):1609-1694. doi: 10.1152/physrev.00045.2024. Epub 2025 Mar 20. Physiol Rev. 2025. PMID: 40111763 Free PMC article. Review.
-
Avoidable deaths in Sweden, 1997-2018: temporal trend and the contribution to the gender gap in life expectancy.BMC Public Health. 2021 Mar 17;21(1):519. doi: 10.1186/s12889-021-10567-5. BMC Public Health. 2021. PMID: 33731076 Free PMC article.
-
Global, regional, and national burden of pancreatic cancer from 1990 to 2021, its attributable risk factors, and projections to 2050: a systematic analysis of the global burden of disease study 2021.BMC Cancer. 2025 Feb 3;25(1):189. doi: 10.1186/s12885-025-13597-z. BMC Cancer. 2025. PMID: 39901108 Free PMC article.
References
-
- GBD 2015 Tobacco Collaborators MB. Fullman N, Ng M, et al. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990–2015: a systematic analysis from the Global Burden of Disease Study 2015. Lancet. 2017;389:1885–1906. doi: 10.1016/S0140-6736(17)30819-X. - DOI - PMC - PubMed
-
- Wang H, Naghavi M, Allen C, et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the global burden of disease study 2015. Lancet. 2016;388:1459–1544. doi: 10.1016/S0140-6736(16)31012-1. - DOI - PMC - PubMed
-
- World Health Organization. WHO report on the global tobacco epidemic, 2017: monitoring tobacco use and prevention policies. https://www.who.int/tobacco/global_report/2017/en/. Accessed 26 Jan 2019.
-
- Lopez AD, Collishaw NE, Piha T. A descriptive model of the cigarette epidemic in developed countries. Tob Control. 1994;3:242–247. doi: 10.1136/tc.3.3.242. - DOI
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
