

Impact of acyclovir use on survival of patients with ventilator-associated pneumonia and high load herpes simplex virus replication
- PMID: 31924246
- PMCID: PMC6954562
- DOI: 10.1186/s13054-019-2701-5
Impact of acyclovir use on survival of patients with ventilator-associated pneumonia and high load herpes simplex virus replication
Abstract
Background: Herpes simplex virus (HSV) replication can be detected in the respiratory secretions of a high proportion of ventilated intensive care unit (ICU) patients. However, the clinical significance remains poorly defined. We investigated whether patients with ventilator-associated pneumonia not responding to antibiotics and in whom high levels of HSV could be detected in respiratory secretions benefit from acyclovir treatment.
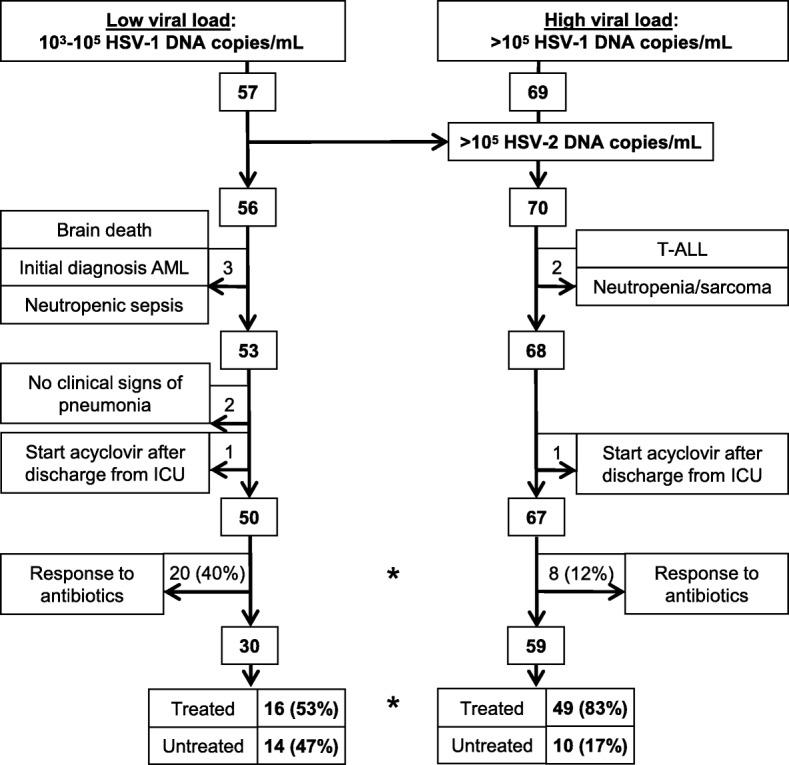
Methods: Respiratory secretions (bronchoalveolar lavage fluid or tracheal aspirates) were tested for HSV replication by quantitative real-time PCR. ICU survival times, clinical parameters, and radiographic findings were retrospectively compared between untreated and acyclovir treated patients with high (> 105 HSV copies/mL) and low (103-105 HSV copies/mL) viral load.
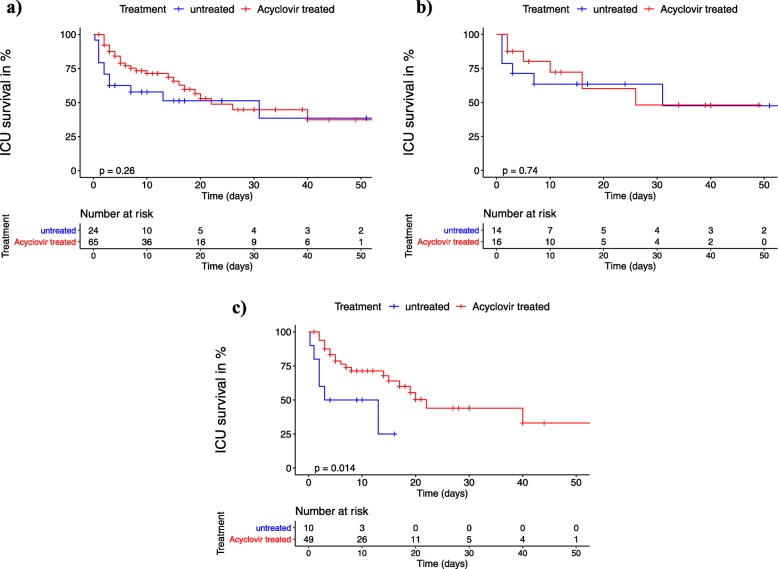
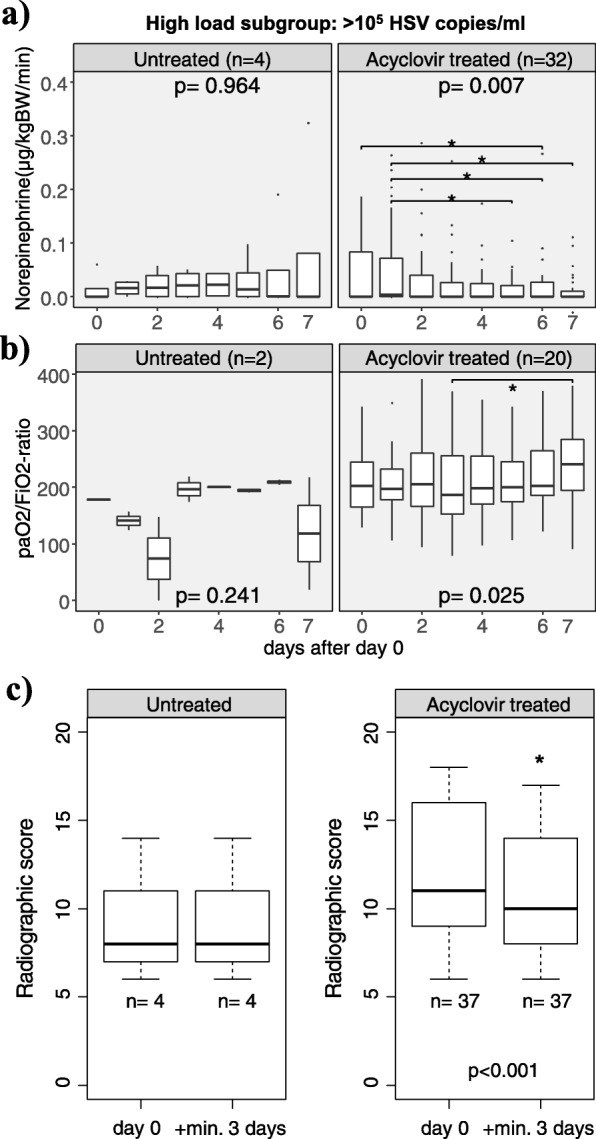
Results: Fifty-seven low and 69 high viral load patients were identified. Fewer patients with high viral load responded to antibiotic treatment (12% compared to 40% of low load patients, p = 0.001). Acyclovir improved median ICU survival (8 vs 22 days, p = 0.014) and was associated with a significantly reduced hazard ratio for ICU death (HR = 0.31, 95% CI 0.11-0.92, p = 0.035) in high load patients only. Moreover, circulatory and pulmonary oxygenation function of high load patients improved significantly over the course of acyclovir treatment: mean norepinephrine doses decreased from 0.05 to 0.02 μg/kg body weight/min between days 0 and 6 of treatment (p = 0.049), and median PaO2/FiO2 ratio increased from 187 to 241 between day 3 and day 7 of treatment (p = 0.02). Chest radiographic findings also improved significantly (p < 0.001).
Conclusions: In patients with ventilator-associated pneumonia, antibiotic treatment failure, and high levels of HSV replication, acyclovir treatment was associated with a significantly longer time to death in the ICU and improved circulatory and pulmonary function. This suggests a causative role for HSV in this highly selected group of patients.
Keywords: Acyclovir; Bronchoalveolar lavage fluid; Real-time polymerase chain reaction; Simplexvirus; Ventilator-associated pneumonia.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Comment in
-
The role of high load herpes simplex virus in patients with mechanical ventilation: a real hospital acquired viral lung infection needs antiviral therapy?Crit Care. 2020 Apr 7;24(1):140. doi: 10.1186/s13054-020-2815-9. Crit Care. 2020. PMID: 32264973 Free PMC article. No abstract available.
-
Acyclovir for ventilator-associated pneumonia refractory to antibiotics and with high viral herpes simplex load: we are not sure.Crit Care. 2020 May 26;24(1):262. doi: 10.1186/s13054-020-02868-9. Crit Care. 2020. PMID: 32456697 Free PMC article. No abstract available.
-
Immortal time bias: a possible explanation for "Impact of acyclovir use on survival of patients with ventilator-associated pneumonia and high load herpes simplex virus replication".Crit Care. 2020 Jun 17;24(1):355. doi: 10.1186/s13054-020-03073-4. Crit Care. 2020. PMID: 32552904 Free PMC article. No abstract available.
Similar articles
-
Cytomegalovirus and herpes simplex virus effect on the prognosis of mechanically ventilated patients suspected to have ventilator-associated pneumonia.PLoS One. 2012;7(12):e51340. doi: 10.1371/journal.pone.0051340. Epub 2012 Dec 7. PLoS One. 2012. Retraction in: PLoS One. 2024 Oct 14;19(10):e0312324. doi: 10.1371/journal.pone.0312324. PMID: 23236477 Free PMC article. Retracted.
-
Is acyclovir effective among critically ill patients with herpes simplex in the respiratory tract?J Clin Virol. 2014 Jul;60(3):215-21. doi: 10.1016/j.jcv.2014.04.010. Epub 2014 Apr 18. J Clin Virol. 2014. PMID: 24800905
-
Effect of acyclovir therapy on the outcome of mechanically ventilated patients with lower respiratory tract infection and detection of herpes simplex virus in bronchoalveolar lavage: protocol for a multicentre, randomised controlled trial (HerpMV).BMJ Open. 2024 Apr 25;14(4):e082512. doi: 10.1136/bmjopen-2023-082512. BMJ Open. 2024. PMID: 38670599 Free PMC article.
-
Herpes simplex encephalitis : from virus to therapy.Infect Disord Drug Targets. 2011 Jun;11(3):235-50. doi: 10.2174/187152611795768088. Infect Disord Drug Targets. 2011. PMID: 21488834 Review.
-
Herpes Simplex Virus Type 1 Pneumonia-A Review.J Intensive Care Med. 2021 Dec;36(12):1398-1402. doi: 10.1177/0885066620965941. Epub 2021 Apr 29. J Intensive Care Med. 2021. PMID: 33926298 Review.
Cited by
-
Effect of antiviral therapy on the outcomes of mechanically ventilated patients with herpes simplex virus detected in the respiratory tract: a systematic review and meta-analysis.Crit Care. 2020 Sep 29;24(1):584. doi: 10.1186/s13054-020-03296-5. Crit Care. 2020. PMID: 32993740 Free PMC article.
-
[Management of infectious complications associated with coronavirus infection in severe patients admitted to ICU].Med Intensiva. 2021 Nov;45(8):485-500. doi: 10.1016/j.medin.2021.04.007. Epub 2021 Apr 30. Med Intensiva. 2021. PMID: 33994616 Free PMC article. Spanish.
-
COVID-associated pulmonary aspergillosis and herpes simplex virus pneumonia in a renal transplant recipient.Transpl Infect Dis. 2022 Dec;24(6):e13978. doi: 10.1111/tid.13978. Epub 2022 Nov 17. Transpl Infect Dis. 2022. PMID: 36306186 Free PMC article. No abstract available.
-
Bronchoscopic suspect of Herpesvirus infection in critically ill COVID-19 patients: two case reports and brief literature review.Acta Biomed. 2022 Jan 19;92(S1):e2021514. doi: 10.23750/abm.v92iS1.12425. Acta Biomed. 2022. PMID: 35045066 Free PMC article.
-
Management of herpesvirus reactivations in patients with solid tumours and hematologic malignancies: update of the Guidelines of the Infectious Diseases Working Party (AGIHO) of the German Society for Hematology and Medical Oncology (DGHO) on herpes simplex virus type 1, herpes simplex virus type 2, and varicella zoster virus.Ann Hematol. 2022 Mar;101(3):491-511. doi: 10.1007/s00277-021-04746-y. Epub 2022 Jan 7. Ann Hematol. 2022. PMID: 34994811 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
