

Proteomic Analysis of CSF from Patients with Leptomeningeal Melanoma Metastases Identifies Signatures Associated with Disease Progression and Therapeutic Resistance
- PMID: 31924735
- PMCID: PMC7196498
- DOI: 10.1158/1078-0432.CCR-19-2840
Proteomic Analysis of CSF from Patients with Leptomeningeal Melanoma Metastases Identifies Signatures Associated with Disease Progression and Therapeutic Resistance
Abstract
Purpose: The development of leptomeningeal melanoma metastases (LMM) is a rare and devastating complication of the late-stage disease, for which no effective treatments exist. Here, we performed a multi-omics analysis of the cerebrospinal fluid (CSF) from patients with LMM to determine how the leptomeningeal microenvironment shapes the biology and therapeutic responses of melanoma cells.
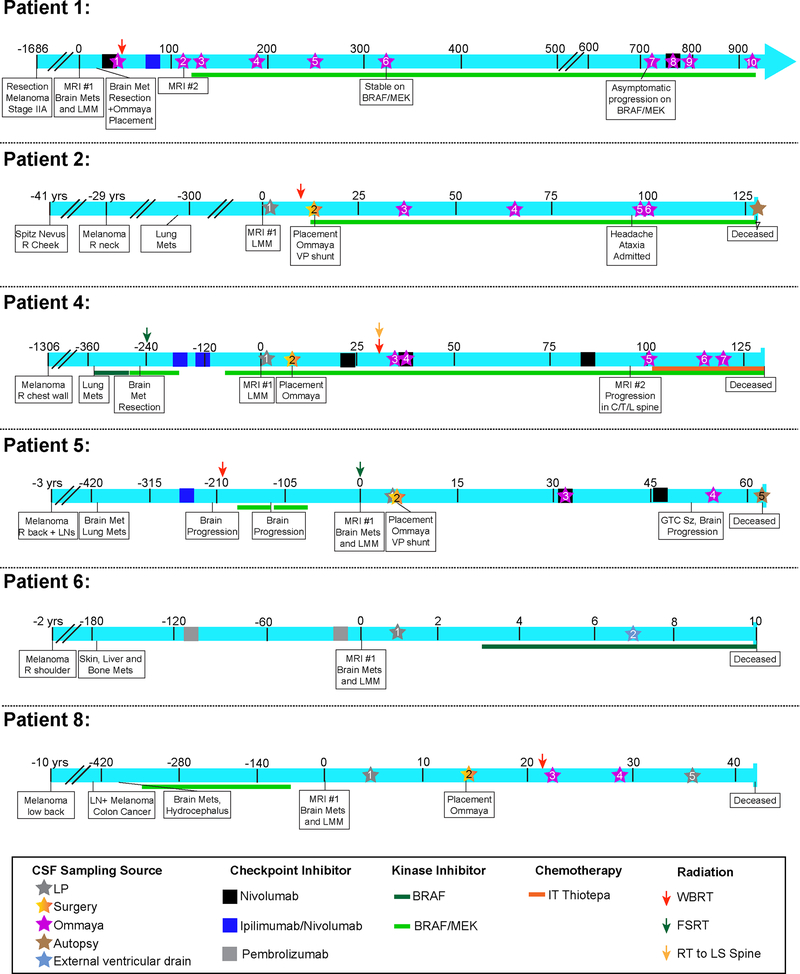
Experimental design: A total of 45 serial CSF samples were collected from 16 patients, 8 of these with confirmed LMM. Of those with LMM, 7 had poor survival (<4 months) and one was an extraordinary responder (still alive with survival >35 months). CSF samples were analyzed by mass spectrometry and incubated with melanoma cells that were subjected to RNA sequencing (RNA-seq) analysis. Functional assays were performed to validate the pathways identified.
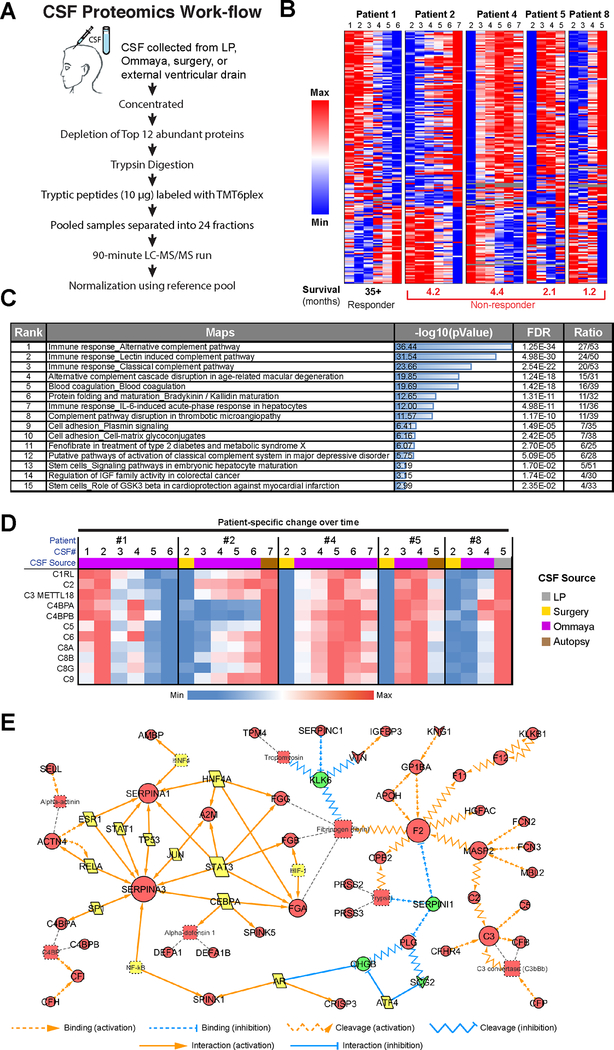
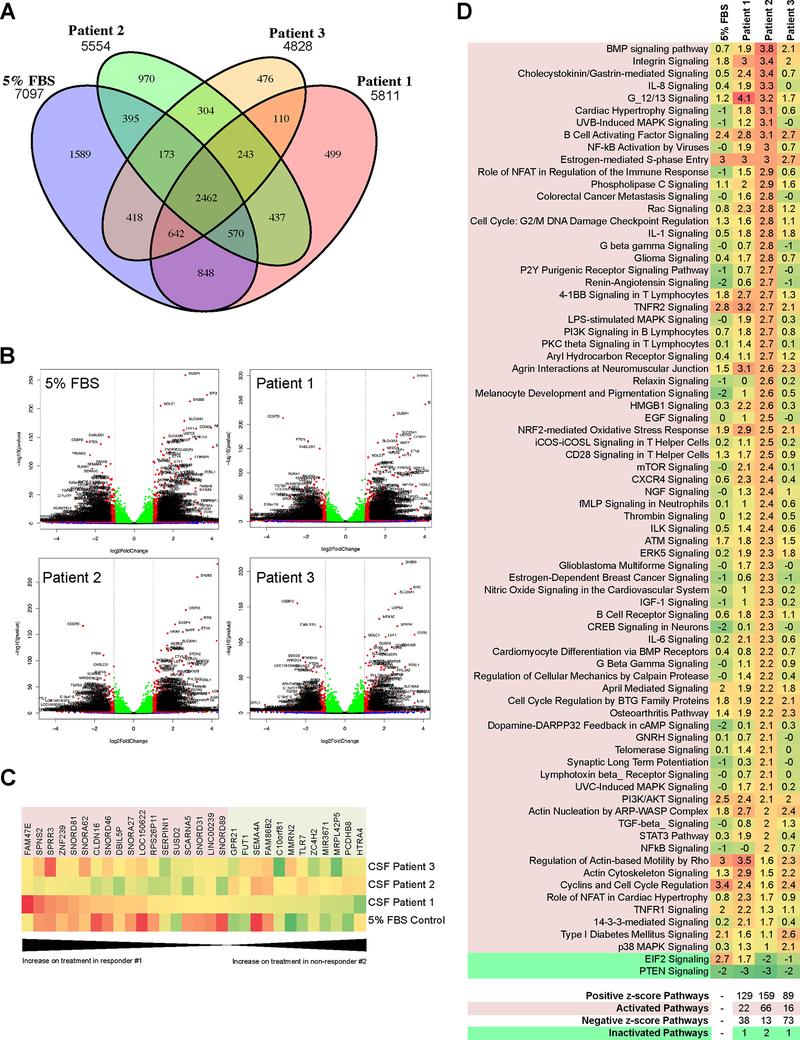
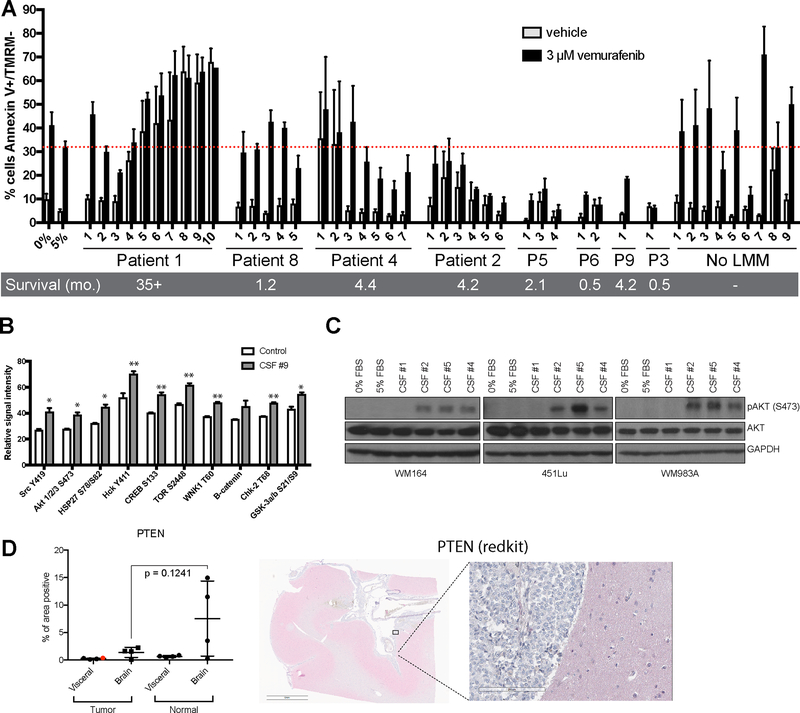
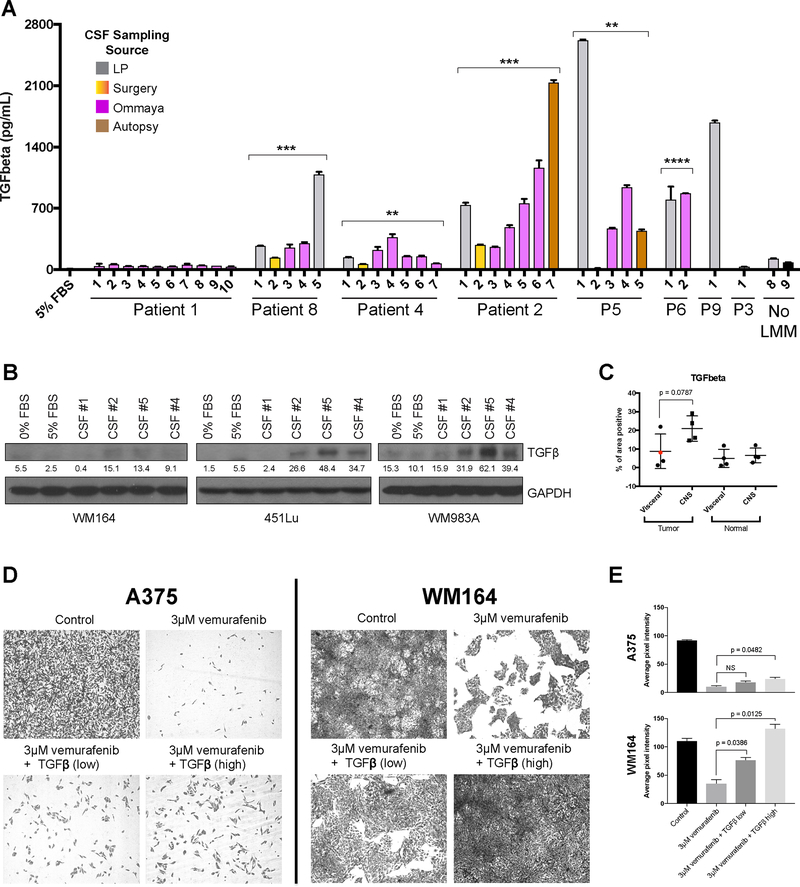
Results: Mass spectrometry analyses showed the CSF of most patients with LMM to be enriched for pathways involved in innate immunity, protease-mediated damage, and IGF-related signaling. All of these were anticorrelated in the extraordinary responder. RNA-seq analysis showed CSF to induce PI3K/AKT, integrin, B-cell activation, S-phase entry, TNFR2, TGFβ, and oxidative stress responses in the melanoma cells. ELISA assays confirmed that TGFβ expression increased in the CSF of patients progressing with LMM. CSF from poorly responding patients conferred tolerance to BRAF inhibitor therapy in apoptosis assays.
Conclusions: These analyses identified proteomic/transcriptional signatures in the CSF of patients who succumbed to LMM. We further showed that the CSF from patients with LMM has the potential to modulate BRAF inhibitor responses and may contribute to drug resistance.See related commentary by Glitza Oliva and Tawbi, p. 2083.
©2020 American Association for Cancer Research.
Conflict of interest statement
Figures
Comment in
-
"Liquid Gold" - The unTAPped Potential of Cerebrospinal Fluid Analysis?Clin Cancer Res. 2020 May 1;26(9):2083-2084. doi: 10.1158/1078-0432.CCR-20-0173. Epub 2020 Mar 5. Clin Cancer Res. 2020. PMID: 32139404 Free PMC article.
Comment on
-
"Liquid Gold" - The unTAPped Potential of Cerebrospinal Fluid Analysis?Clin Cancer Res. 2020 May 1;26(9):2083-2084. doi: 10.1158/1078-0432.CCR-20-0173. Epub 2020 Mar 5. Clin Cancer Res. 2020. PMID: 32139404 Free PMC article.
References
-
- Kokkoris CP. Leptomeningeal carcinomatosis. How does cancer reach the pia-arachnoid? Cancer 1983;51(1):154–60. - PubMed
-
- Pape E, Desmedt E, Zairi F, Baranzelli MC, Dziwniel V, Dubois F, et al. Leptomeningeal metastasis in melanoma: a prospective clinical study of nine patients. In Vivo 2012;26(6):1079–86. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
