

Clonal kinetics and single-cell transcriptional profiling of CAR-T cells in patients undergoing CD19 CAR-T immunotherapy
- PMID: 31924795
- PMCID: PMC6954177
- DOI: 10.1038/s41467-019-13880-1
Clonal kinetics and single-cell transcriptional profiling of CAR-T cells in patients undergoing CD19 CAR-T immunotherapy
Abstract
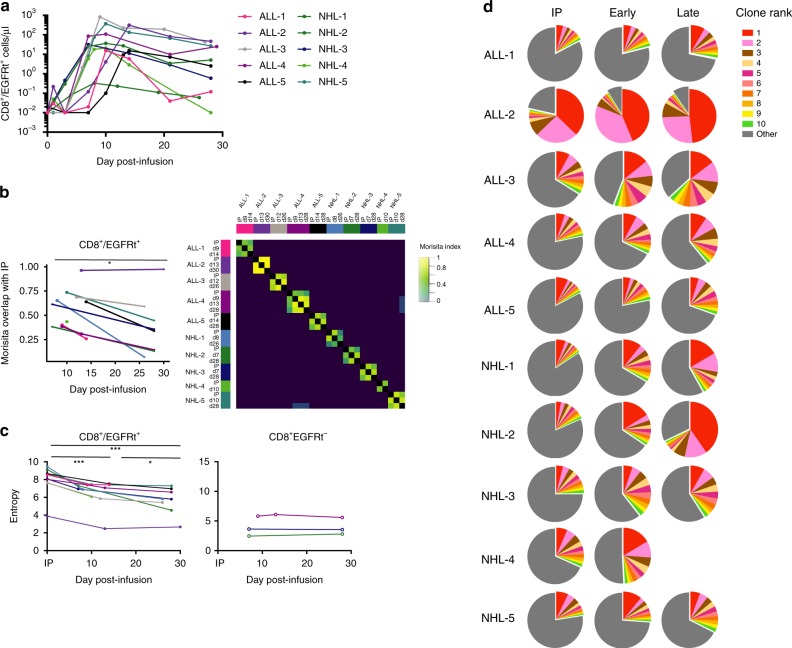
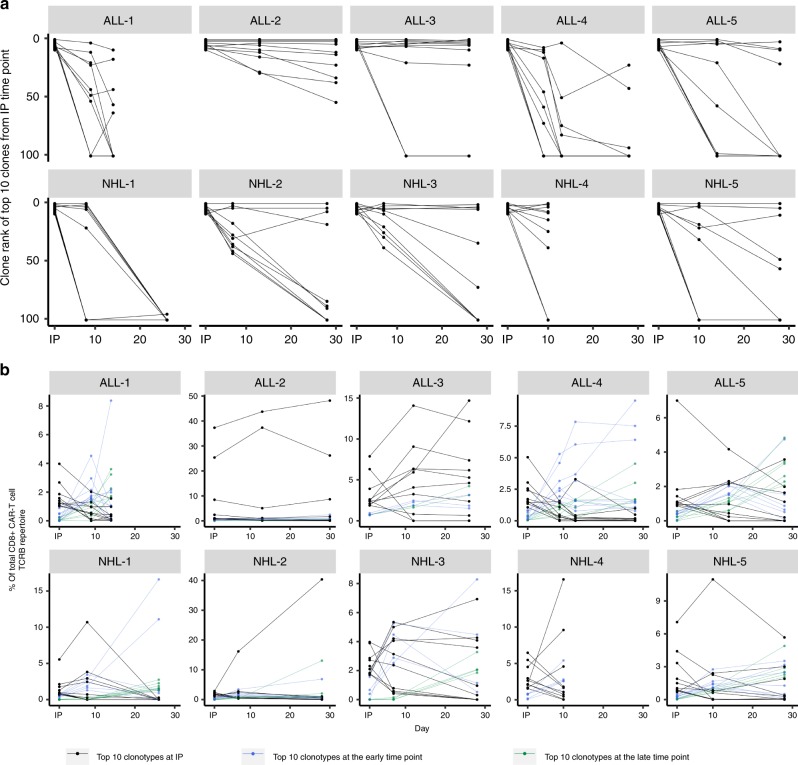
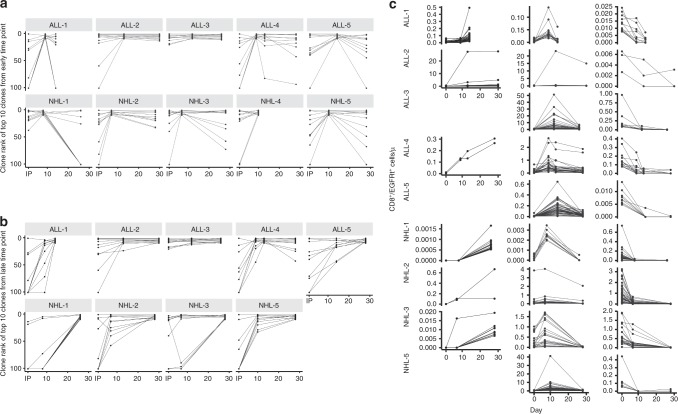
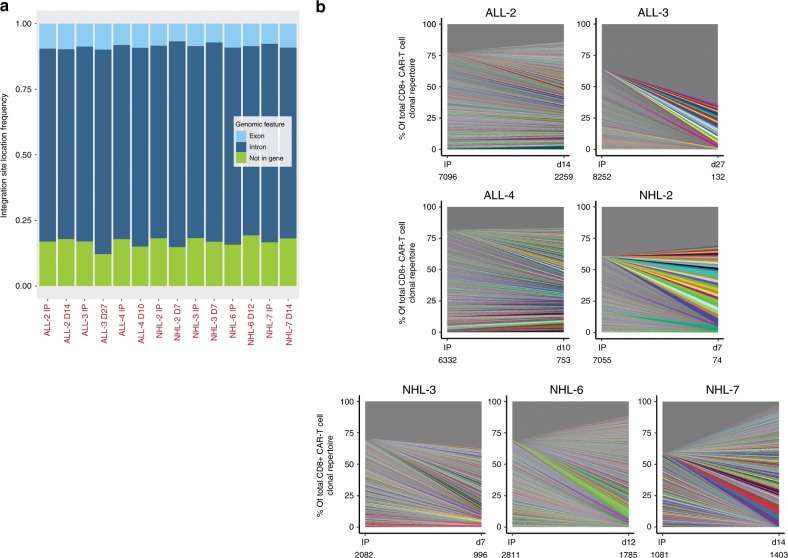
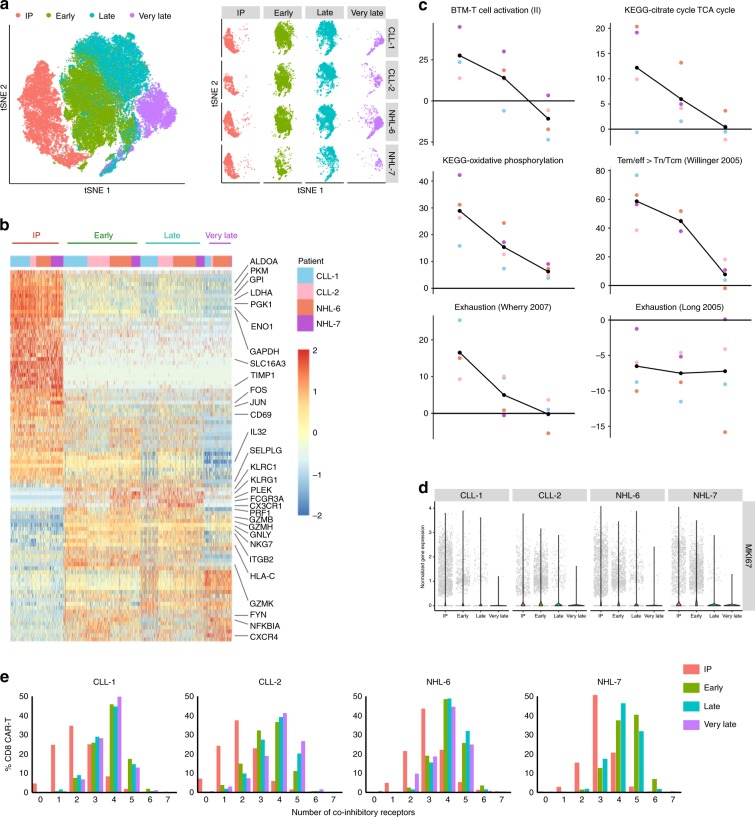
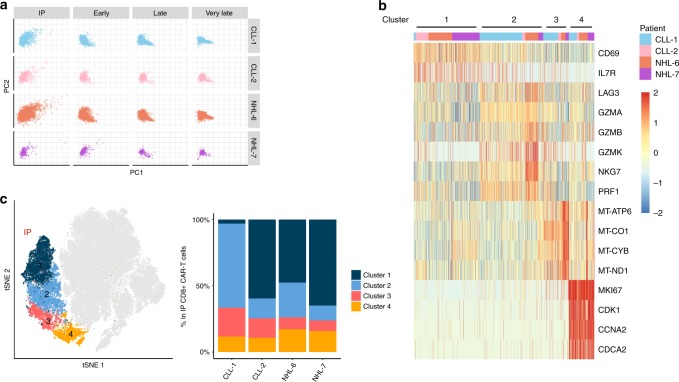
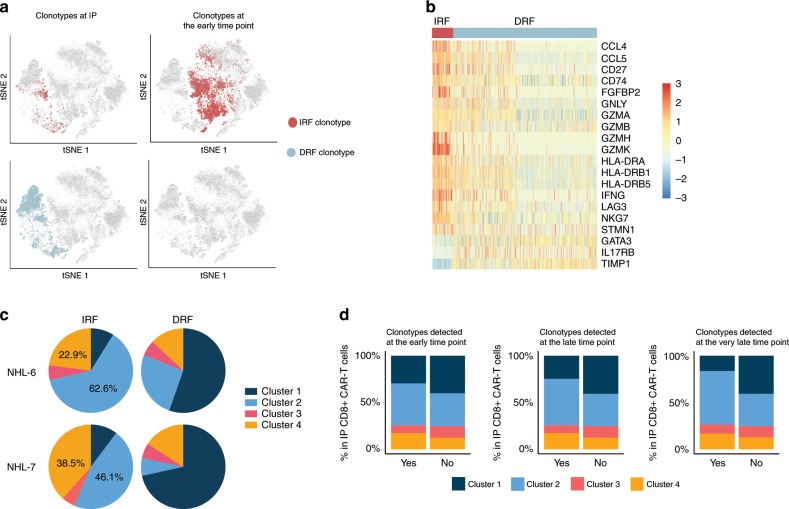
Chimeric antigen receptor (CAR) T-cell therapy has produced remarkable anti-tumor responses in patients with B-cell malignancies. However, clonal kinetics and transcriptional programs that regulate the fate of CAR-T cells after infusion remain poorly understood. Here we perform TCRB sequencing, integration site analysis, and single-cell RNA sequencing (scRNA-seq) to profile CD8+ CAR-T cells from infusion products (IPs) and blood of patients undergoing CD19 CAR-T immunotherapy. TCRB sequencing shows that clonal diversity of CAR-T cells is highest in the IPs and declines following infusion. We observe clones that display distinct patterns of clonal kinetics, making variable contributions to the CAR-T cell pool after infusion. Although integration site does not appear to be a key driver of clonal kinetics, scRNA-seq demonstrates that clones that expand after infusion mainly originate from infused clusters with higher expression of cytotoxicity and proliferation genes. Thus, we uncover transcriptional programs associated with CAR-T cell behavior after infusion.
Conflict of interest statement
S.R.R. received research funding from Juno Therapeutics, a Celgene company, has patents licensed to Juno Therapeutics, a Celgene company, has equity ownership in Celgene, and has served on advisory boards for Adaptive Biotechnologies, Cell Medica, Juno Therapeutics, a Celgene company, and NOHLA. D.G.M. received research funding from GlaxoSmithKline and Juno Therapeutics, a Celgene company. H.P.K. is a consultant to and has ownership interests with Rocket Pharma and Homology Medicines, is a consultant to CSL Behring and Magenta Therapeutics, and is an inventor on patent applications (#62/351,761, #62/428,994, and #PCT/US2017/037967) submitted by the Fred Hutchinson Cancer Research Center that cover the selection and use of cell populations for research and therapeutic purposes, as well as strategies to assess and/or produce cell populations with predictive engraftment potential. C.J.T. received research funding from Juno Therapeutics, a Celgene company, and Nektar Therapeutics, has patents licensed to Juno Therapeutics, a Celgene company, has served on advisory boards, has equity ownership in Caribou Biosciences, Eureka Therapeutics, and Precision Biosciences, and has served on advisory boards for Aptevo, Juno Therapeutics, a Celgene company, Kite, a Gilead Company, Nektar Therapeutics, Novartis, Allogene, Myeloid Therapeutics, and PACT Pharma. R.G. has received consulting income from Juno Therapeutics, Takeda, Infotech Soft, Celgene, has received research support from Janssen Pharmaceuticals and Juno Therapeutics, and declares ownership in Cellspace Biosciences. The remaining authors declare no competing financial interests. Companies funding this research did not have any role in the study design or data analysis and interpretation.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
