

Clinical relevance of systemic monocytic-MDSCs in patients with metastatic breast cancer
- PMID: 31925475
- PMCID: PMC7044142
- DOI: 10.1007/s00262-019-02472-z
Clinical relevance of systemic monocytic-MDSCs in patients with metastatic breast cancer
Abstract
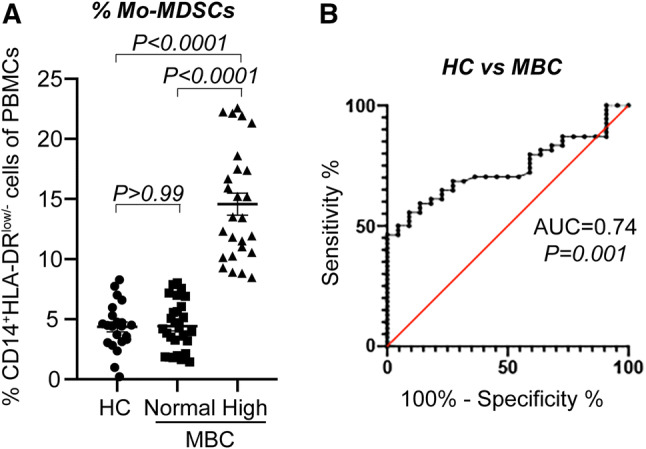
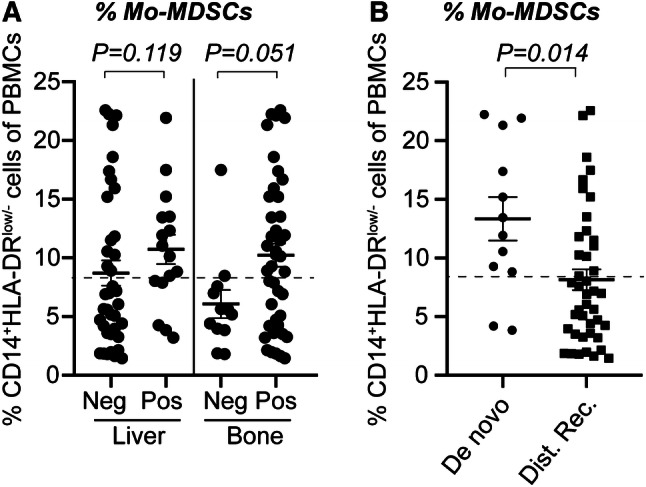
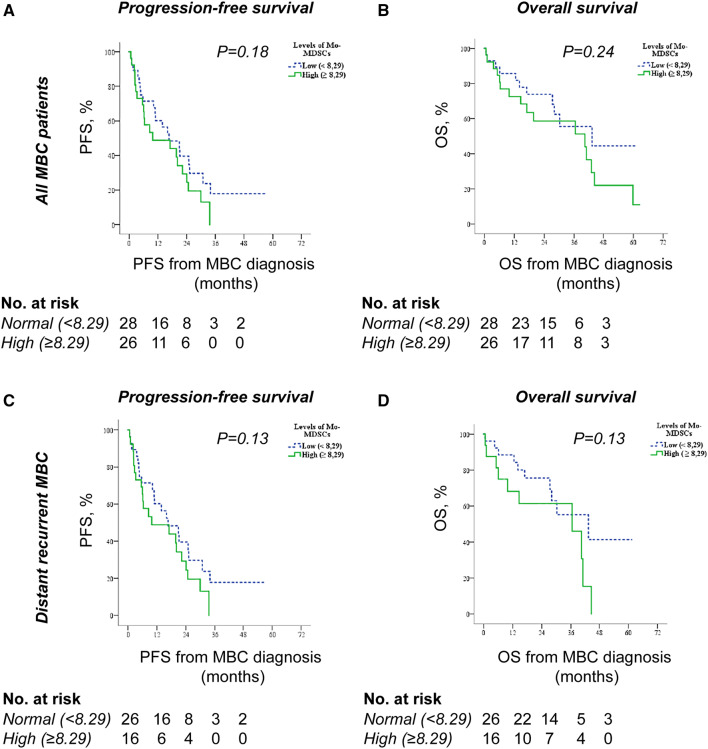
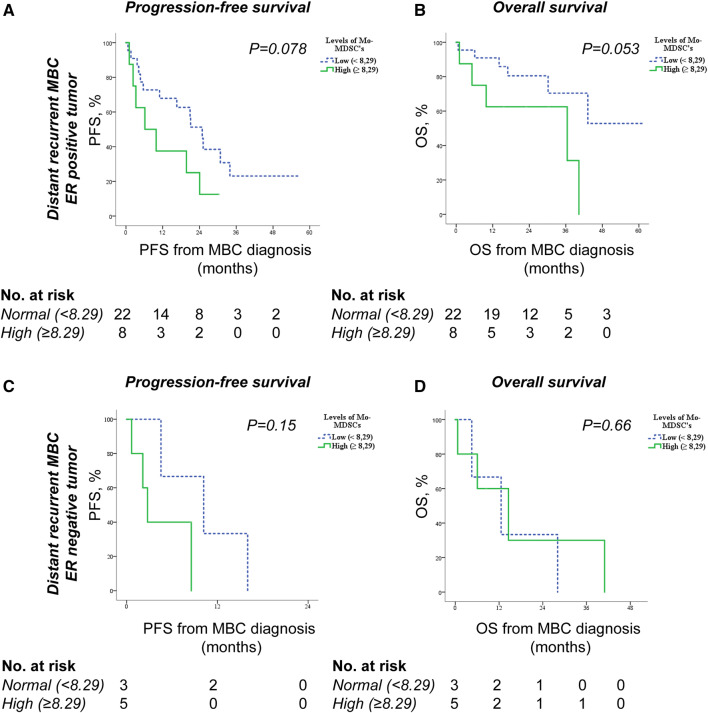
The overall aim of this prospective study was to delineate the role of monocytic myeloid-derived suppressor cells (Mo-MDSCs) in patients with metastatic breast cancer (MBC). MDSCs are a heterogeneous group of immunosuppressive cells often enriched in different malignancies which hold prognostic and predictive value for clinical outcomes. Here, we assessed the clinical significance of Mo-MDSCs in 54 patients with de novo or distant recurrent MBC. We show that high levels of Mo-MDSCs significantly correlated with de novo MBC (metastatic disease at initial diagnosis), estrogen receptor (ER) negativity, and liver- and bone metastasis. A trend towards an association between high levels of Mo-MDSCs and survival (P = 0.053) was also found in patients with distant recurrent ER-positive MBC. We therefore propose that an increased population of Mo-MDSCs may be related to the metastatic or immunoregulatory switch associated with transition to a more systemic disease. Our data imply that high levels of systemic Mo-MDSCs represent patients with more aggressive disease and worse outcome.
Keywords: Breast cancer; Estrogen receptor; Metastasis; Mo-MDSCs; Survival.
Conflict of interest statement
The authors declare no conflict of interests.
Figures
Similar articles
-
Systemic Monocytic-MDSCs Are Generated from Monocytes and Correlate with Disease Progression in Breast Cancer Patients.PLoS One. 2015 May 20;10(5):e0127028. doi: 10.1371/journal.pone.0127028. eCollection 2015. PLoS One. 2015. PMID: 25992611 Free PMC article.
-
Increased Percentage of mo-MDSCs in Human Peripheral Blood May Be a Potential Indicator in the Diagnosis of Breast Cancer.Oncol Res Treat. 2017;40(10):603-608. doi: 10.1159/000478933. Epub 2017 Sep 12. Oncol Res Treat. 2017. PMID: 28892809
-
Visualization and quantification of in vivo homing kinetics of myeloid-derived suppressor cells in primary and metastatic cancer.Theranostics. 2019 Aug 12;9(20):5869-5885. doi: 10.7150/thno.33275. eCollection 2019. Theranostics. 2019. PMID: 31534525 Free PMC article.
-
[Roles of Myeloid-derived Suppressor Cells in Breast Cancer Metastasis].Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2021 Jun 30;43(3):445-451. doi: 10.3881/j.issn.1000-503X.12586. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2021. PMID: 34238422 Review. Chinese.
-
Suppressive role of myeloid-derived suppressor cells (MDSCs) in the microenvironment of breast cancer and targeted immunotherapies.Oncotarget. 2016 Sep 27;7(39):64505-64511. doi: 10.18632/oncotarget.11352. Oncotarget. 2016. PMID: 27542274 Free PMC article. Review.
Cited by
-
Peripheral Blood Classical Monocytes and Plasma Interleukin 10 Are Associated to Neoadjuvant Chemotherapy Response in Breast Cancer Patients.Front Immunol. 2020 Jul 9;11:1413. doi: 10.3389/fimmu.2020.01413. eCollection 2020. Front Immunol. 2020. PMID: 32733470 Free PMC article.
-
Phenotypic Analysis of Circulating Myeloid Derived Suppressor Cells and Their Subpopulations in Egyptian Females with Breast Cancer: A Single-Centre Case-Control Study.Asian Pac J Cancer Prev. 2024 Jan 1;25(1):257-263. doi: 10.31557/APJCP.2024.25.1.257. Asian Pac J Cancer Prev. 2024. PMID: 38285792 Free PMC article.
-
GB1275, a first-in-class CD11b modulator: rationale for immunotherapeutic combinations in solid tumors.J Immunother Cancer. 2021 Aug;9(8):e003005. doi: 10.1136/jitc-2021-003005. J Immunother Cancer. 2021. PMID: 34452928 Free PMC article. Review.
-
Circulating inflammatory cells in patients with metastatic breast cancer: Implications for treatment.Front Oncol. 2022 Aug 8;12:882896. doi: 10.3389/fonc.2022.882896. eCollection 2022. Front Oncol. 2022. PMID: 36003772 Free PMC article. Review.
-
Obesity correlates with the immunosuppressive ILC2s-MDSCs axis in advanced breast cancer.Immun Inflamm Dis. 2024 Mar;12(3):e1196. doi: 10.1002/iid3.1196. Immun Inflamm Dis. 2024. PMID: 38501542 Free PMC article.
References
-
- Bray Freddie, Ferlay Jacques, Soerjomataram Isabelle, Siegel Rebecca L., Torre Lindsey A., Jemal Ahmedin. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer Journal for Clinicians. 2018;68(6):394–424. - PubMed
-
- SweBCG (2018) Swedish Breast Cancer Group national guidelines. Available from http://www.swebcg.se
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
