

Clinical pharmacokinetics of 3-h extended infusion of meropenem in adult patients with severe sepsis and septic shock: implications for empirical therapy against Gram-negative bacteria
- PMID: 31925610
- PMCID: PMC6954163
- DOI: 10.1186/s13613-019-0622-8
Clinical pharmacokinetics of 3-h extended infusion of meropenem in adult patients with severe sepsis and septic shock: implications for empirical therapy against Gram-negative bacteria
Abstract
Background: Optimal anti-bacterial activity of meropenem requires maintenance of its plasma concentration (Cp) above the minimum inhibitory concentration (MIC) of the pathogen for at least 40% of the dosing interval (fT > MIC > 40). We aimed to determine whether a 3-h extended infusion (EI) of meropenem achieves fT > MIC > 40 on the first and third days of therapy in patients with severe sepsis or septic shock. We also simulated the performance of the EI with respect to other pharmacokinetic (PK) targets such as fT > 4 × MIC > 40, fT > MIC = 100, and fT > 4 × MIC = 100.
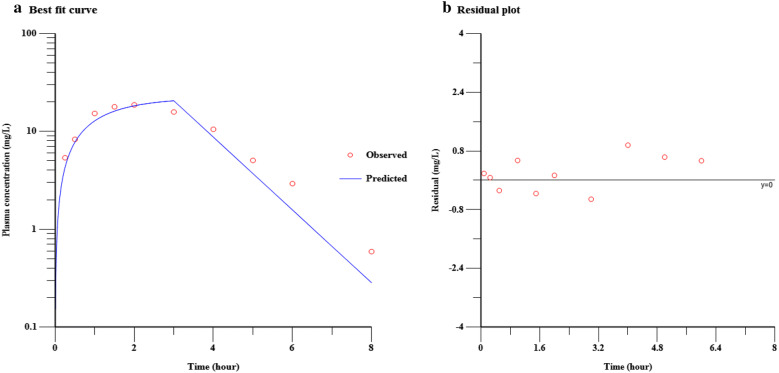
Methods: Arterial blood samples of 25 adults with severe sepsis or septic shock receiving meropenem 1000 mg as a 3-h EI eight hourly (Q8H) were obtained at various intervals during and after the first and seventh doses. Plasma meropenem concentrations were determined using a reverse-phase high-performance liquid chromatography assay, followed by modeling and simulation of PK data. European Committee on Antimicrobial Susceptibility Testing (EUCAST) definitions of MIC breakpoints for sensitive and resistant Gram-negative bacteria were used.
Results: A 3-h EI of meropenem 1000 mg Q8H achieved fT > 2 µg/mL > 40 on the first and third days, providing activity against sensitive strains of Enterobacteriaceae, Pseudomonas aeruginosa and Acinetobacter baumannii. However, it failed to achieve fT > 4 µg/mL > 40 to provide activity against strains susceptible to increased exposure in 33.3 and 39.1% patients on the first and the third days, respectively. Modeling and simulation showed that a bolus dose of 500 mg followed by 3-h EI of meropenem 1500 mg Q8H will achieve this target. A bolus of 500 mg followed by an infusion of 2000 mg would be required to achieve fT > 8 µg > 40. Targets of fT > 4 µg/mL = 100 and fT > 8 µg/mL = 100 may be achievable in two-thirds of patients by increasing the frequency of dosing to six hourly (Q6H).
Conclusions: In patients with severe sepsis or septic shock, EI of 1000 mg of meropenem over 3 h administered Q8H is inadequate to provide activity (fT > 4 µg/mL > 40) against strains susceptible to increased exposure, which requires a bolus of 500 mg followed by EI of 1500 mg Q8H. While fT > 8 µg/mL > 40 require escalation of EI dose, fT > 4 µg/mL = 100 and fT > 8 µg/mL = 100 require escalation of both EI dose and frequency.
Keywords: Anti-bacterial agents; Antimicrobial pharmacokinetics; Meropenem dosing; Septic shock.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Optimized meropenem dosage regimens using a pharmacokinetic/pharmacodynamic population approach in patients undergoing continuous venovenous haemodiafiltration with high-adsorbent membrane.J Antimicrob Chemother. 2019 Oct 1;74(10):2979-2983. doi: 10.1093/jac/dkz299. J Antimicrob Chemother. 2019. PMID: 31335959
-
Comparison of two empirical prolonged infusion dosing regimens for meropenem in patients with septic shock: A two-center pilot study.Int J Antimicrob Agents. 2021 Mar;57(3):106289. doi: 10.1016/j.ijantimicag.2021.106289. Epub 2021 Jan 27. Int J Antimicrob Agents. 2021. PMID: 33515688
-
Defining Exposure Predictors of Meropenem That Are Associated with Improved Survival for Severe Bacterial Infection: A Preclinical PK/PD Study in Sepsis Rat Model.Antibiotics (Basel). 2022 Nov 19;11(11):1660. doi: 10.3390/antibiotics11111660. Antibiotics (Basel). 2022. PMID: 36421304 Free PMC article.
-
Cefiderocol: A Siderophore Cephalosporin with Activity Against Carbapenem-Resistant and Multidrug-Resistant Gram-Negative Bacilli.Drugs. 2019 Feb;79(3):271-289. doi: 10.1007/s40265-019-1055-2. Drugs. 2019. PMID: 30712199 Review.
-
Evaluation of studies on extended versus standard infusion of beta-lactam antibiotics.Am J Health Syst Pharm. 2019 Sep 3;76(18):1383-1394. doi: 10.1093/ajhp/zxz154. Am J Health Syst Pharm. 2019. PMID: 31505562 Review.
Cited by
-
Pharmacokinetics and Monte Carlo Simulation of Meropenem in Critically Ill Adult Patients Receiving Extracorporeal Membrane Oxygenation.Front Pharmacol. 2021 Nov 1;12:768912. doi: 10.3389/fphar.2021.768912. eCollection 2021. Front Pharmacol. 2021. PMID: 34790131 Free PMC article.
-
Evaluation of Empirical Meropenem Bolus Protocol in Pseudomonas aeruginosa: A Three-Year Analysis in Tertiary Intensive Care Unit.Int J Gen Med. 2021 Nov 9;14:7861-7867. doi: 10.2147/IJGM.S341423. eCollection 2021. Int J Gen Med. 2021. PMID: 34795507 Free PMC article.
-
Chinese ICU physicians' knowledge of antibiotic pharmacokinetics/pharmacodynamics (PK/PD): a cross-sectional survey.BMC Med Educ. 2022 Mar 14;22(1):173. doi: 10.1186/s12909-022-03234-9. BMC Med Educ. 2022. PMID: 35287666 Free PMC article.
-
Precision Dosing of Meropenem in Adults with Normal Renal Function: Insights from a Population Pharmacokinetic and Monte Carlo Simulation Study.Antibiotics (Basel). 2024 Sep 5;13(9):849. doi: 10.3390/antibiotics13090849. Antibiotics (Basel). 2024. PMID: 39335022 Free PMC article.
-
Comparison between meropenem and ceftolozane/tazobactam: possible influence of CRRT.Crit Care. 2022 Jan 7;26(1):15. doi: 10.1186/s13054-021-03837-6. Crit Care. 2022. PMID: 34996512 Free PMC article. No abstract available.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
