

Ultrasonographic characterization of lingual structures pertinent to oral, periodontal, and implant surgery
- PMID: 31925829
- PMCID: PMC7959268
- DOI: 10.1111/clr.13573
Ultrasonographic characterization of lingual structures pertinent to oral, periodontal, and implant surgery
Abstract
Objectives: Increased applications of ridge augmentation in the lingual posterior mandible call for an urgent need to study its anatomy. Therefore, our first aim was to validate ultrasound in measuring the mandibular lingual structures in human cadavers. Secondarily, to test its feasibility in imaging the lingual nerve in live humans.
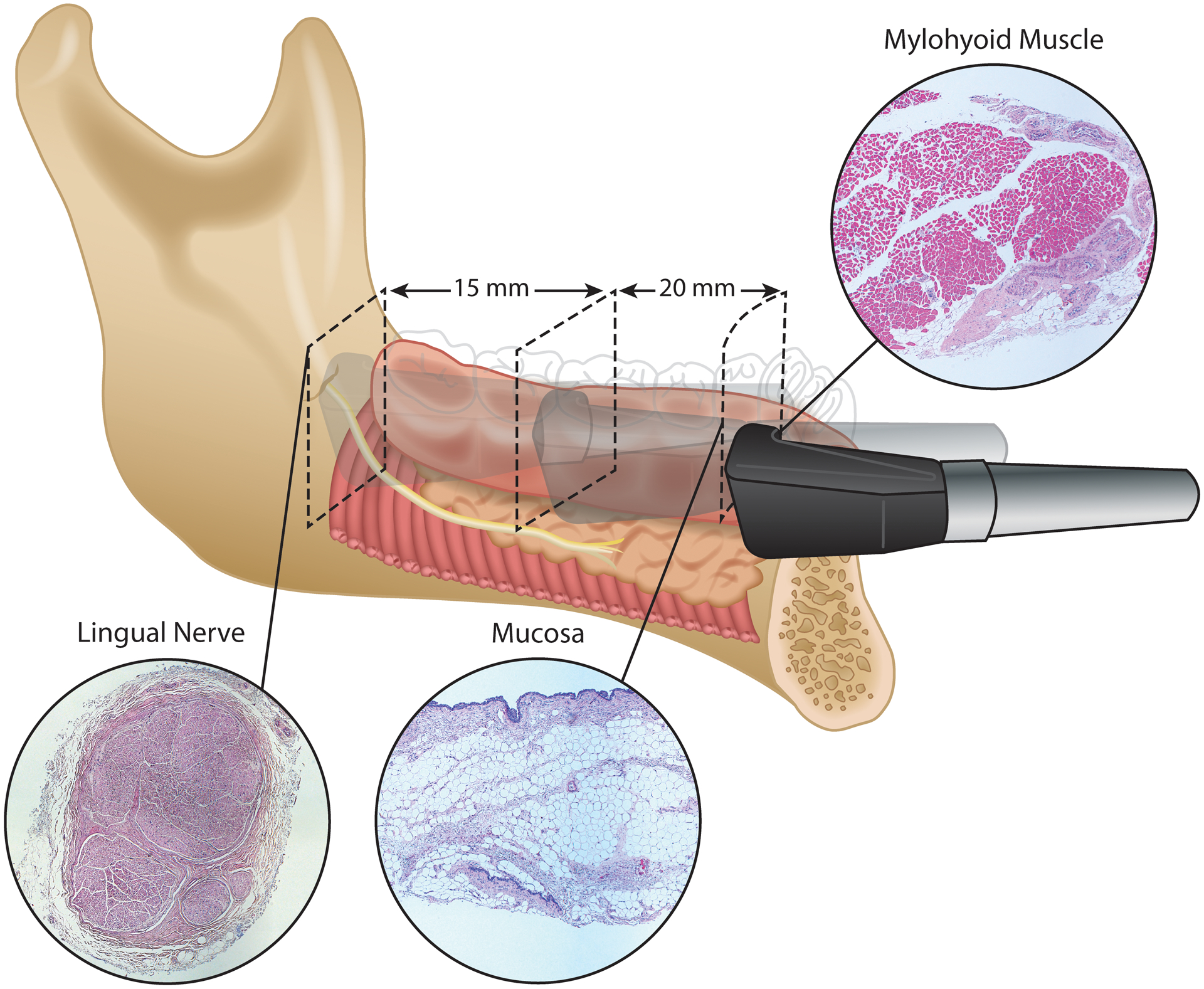
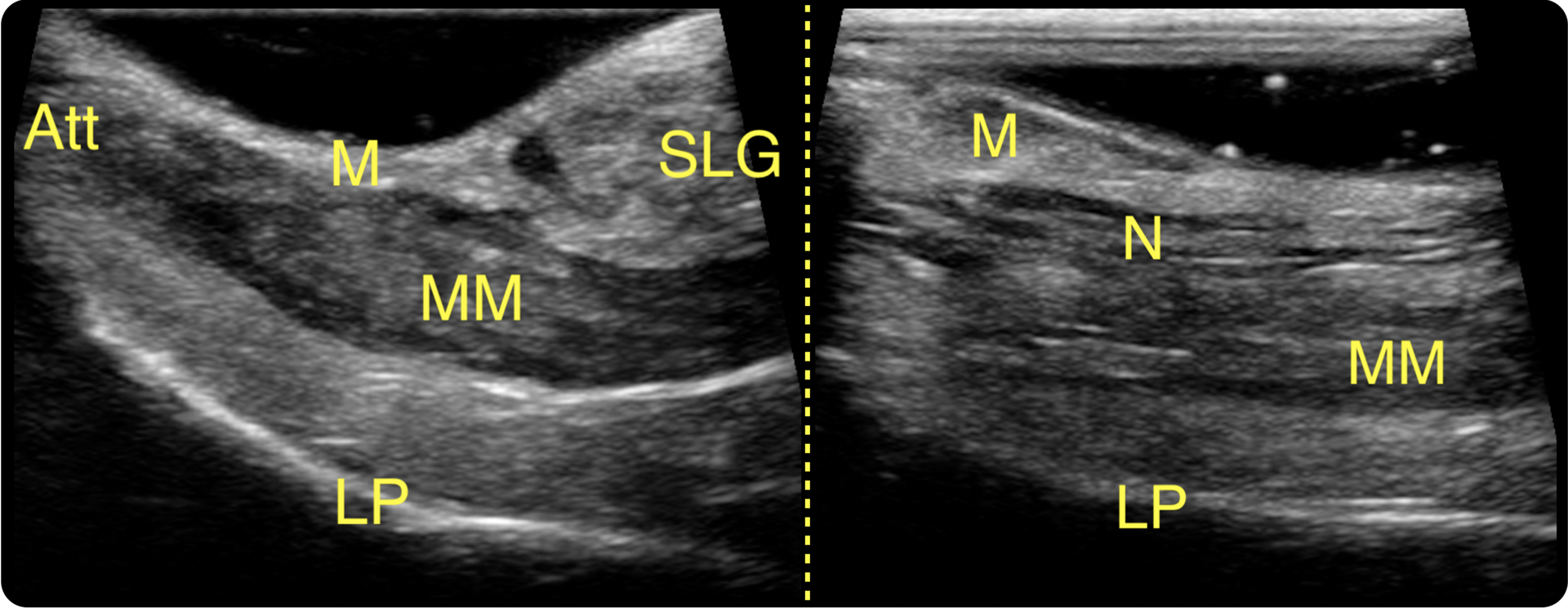
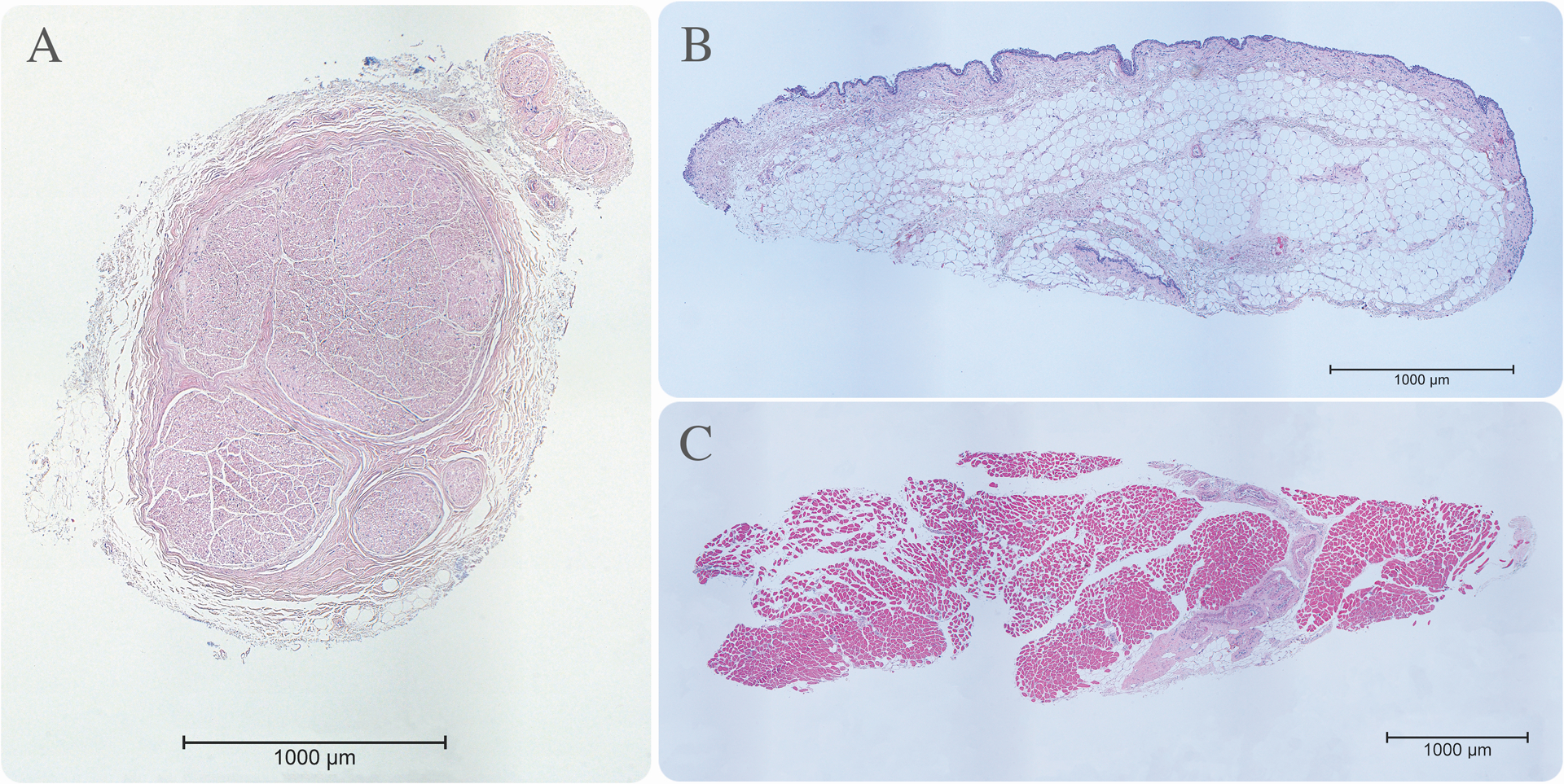
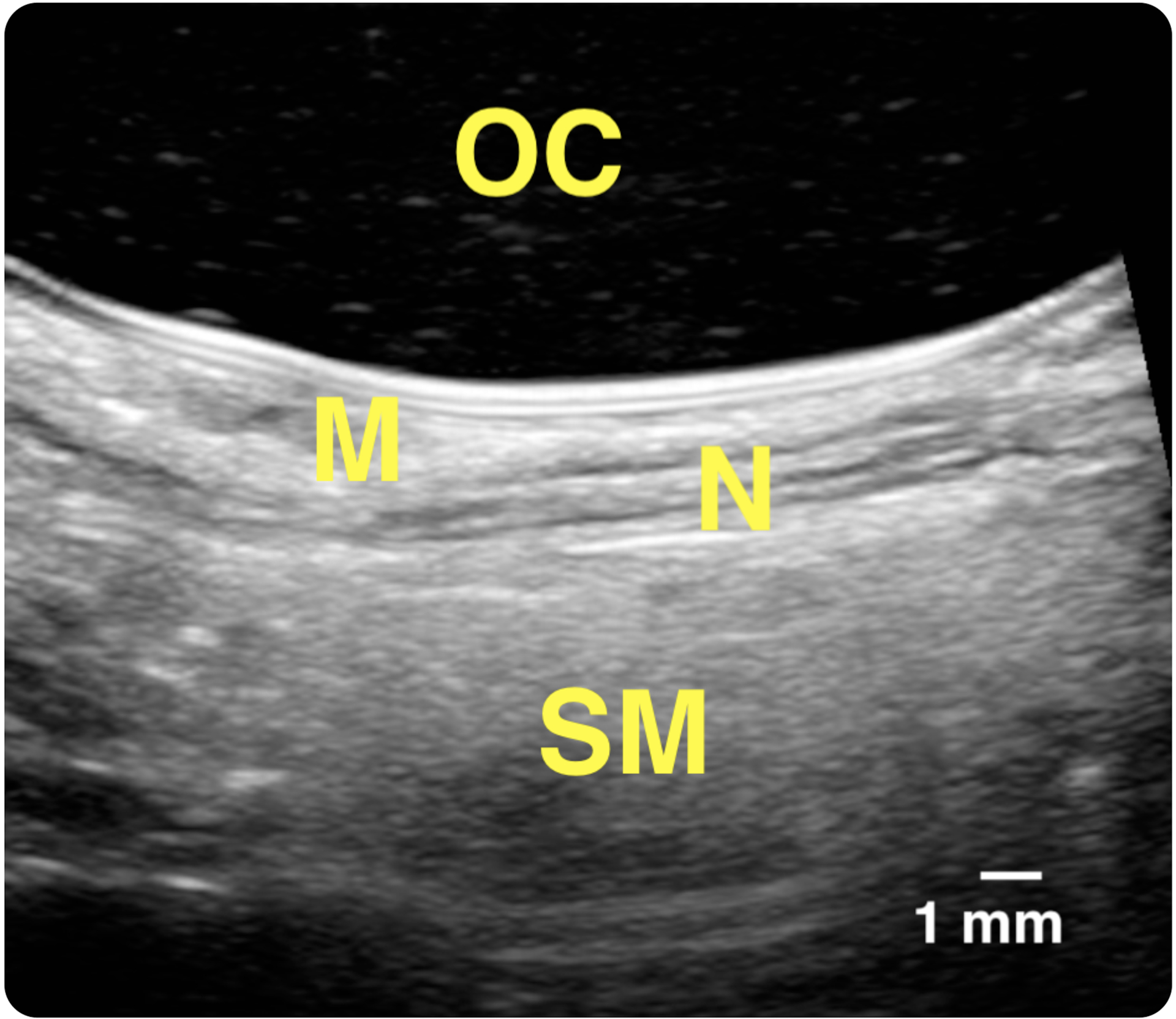
Materials and methods: Nine fresh un-embalmed fully/partially edentulous cadaver heads were utilized for aim 1. Three areas in the lingual mandible were imaged (mandibular premolar, molar, and retromolar). Immediately after, biopsies were harvested from each site. The thickness of the mucosa, mylohyoid muscle, and lingual nerve diameter was measured via ultrasound and statistically compared to histology. Similarly, the lingual nerve in live humans was also imaged.
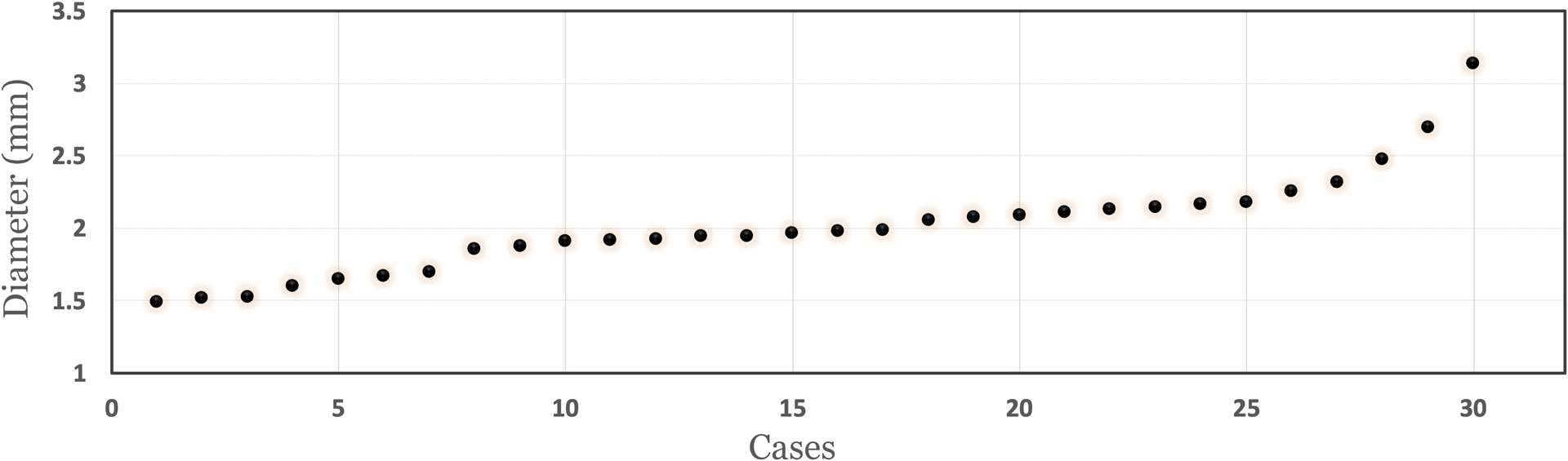
Results: None of the differences between the ultrasound and histology measurements reached statistical significance (p > .05). The mean mucosal thickness via ultrasound and histology was 1.45 ± 0.49 and 1.39 ± 0.50 mm, 5 mm lingual to the mylohyoid muscle attachment. At 10 mm beyond the attachment, the ultrasound and histologic values were 1.54 ± 0.48 and 1.37 ± 0.49, respectively. The mean muscle thickness measured via ultrasound and histology was 2.31 ± 0.56 and 2.25 ± 0.47 mm, at the 5 mm distance. At the 10 mm distance, the measurements were 2.46 ± 0.56 and 2.36 ± 0.5 mm, respectively. The mean ultrasonic lingual nerve diameter was 2.38 ± 0.44 mm, versus 2.43 ± 0.42 mm, with histology. The lingual nerve diameter on 19 live humans averaged to 2.01 ± 0.35 mm (1.4-3.1 mm).
Conclusions: Within its limitations, ultrasound accurately measured mandibular lingual soft tissue structures on cadavers, and the lingual nerve on live humans.
Keywords: alveolar ridge; anatomy; dental implant; diagnosis; ultrasonography.
© 2020 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd.
Conflict of interest statement
Conflict of interest:
The authors do not have any financial interests, either directly or indirectly, in the products or information listed in the paper. The study was supported by grants from the Delta Dental Foundation (PAF01878), the Osteology Foundation (PAF06301), Department of Periodontics and Oral Medicine Clinical Research Supplemental Research Grant, School of Dentistry Research Collaborative Award (U054647) and a NIDCR grant (1R21DE027765).
Figures
References
-
- Annibali S, Ripari M, La Monaca G, Tonoli F, & Cristalli MP (2009). Local accidents in dental implant surgery: prevention and treatment. Int J Periodontics Restorative Dent, 29(3), 325–331. - PubMed
-
- Balasubramanian S, Paneerselvam E, Guruprasad T, Pathumai M, Abraham S, & Krishnakumar Raja VB (2017). Efficacy of Exclusive Lingual Nerve Block versus Conventional Inferior Alveolar Nerve Block in Achieving Lingual Soft-tissue Anesthesia. Ann Maxillofac Surg, 7(2), 250–255. doi: 10.4103/ams.ams_65_17 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
