

Design, Implementation, and in Vivo Validation of a Novel Proton FLASH Radiation Therapy System
- PMID: 31928642
- PMCID: PMC7325740
- DOI: 10.1016/j.ijrobp.2019.10.049
Design, Implementation, and in Vivo Validation of a Novel Proton FLASH Radiation Therapy System
Abstract
Purpose: Recent studies suggest that ultrahigh-dose-rate, "FLASH," electron radiation therapy (RT) decreases normal tissue damage while maintaining tumor response compared with conventional dose rate RT. Here, we describe a novel RT apparatus that delivers FLASH proton RT (PRT) using double scattered protons with computed tomography guidance and provide the first report of proton FLASH RT-mediated normal tissue radioprotection.
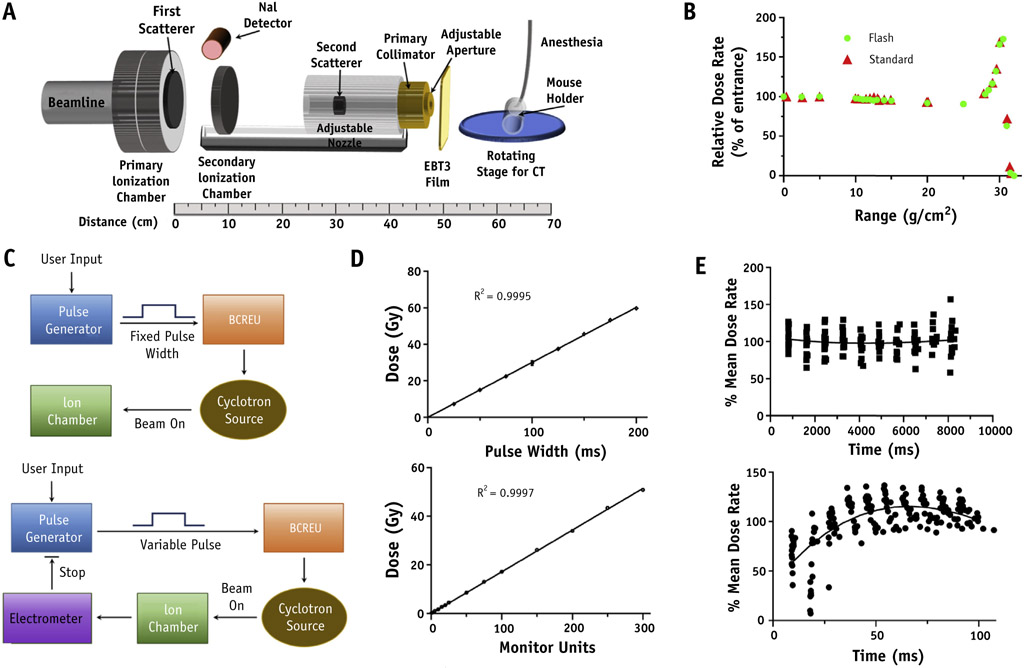
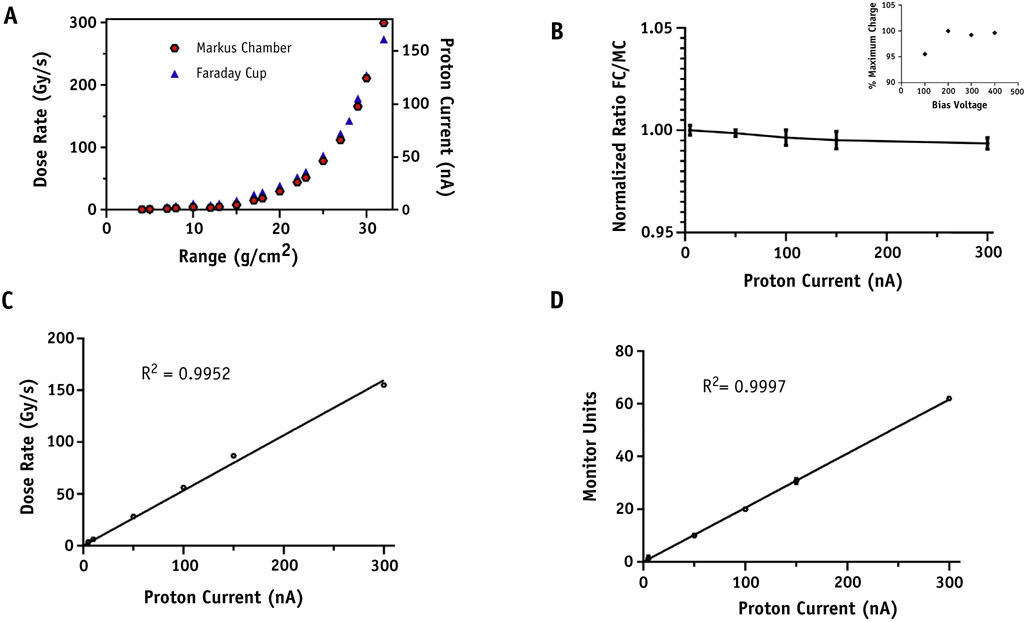
Methods and materials: Absolute dose was measured at multiple depths in solid water and validated against an absolute integral charge measurement using a Faraday cup. Real-time dose rate was obtained using a NaI detector to measure prompt gamma rays. The effect of FLASH versus standard dose rate PRT on tumors and normal tissues was measured using pancreatic flank tumors (MH641905) derived from the KPC autochthonous PanCa model in syngeneic C57BL/6J mice with analysis of fibrosis and stem cell repopulation in small intestine after abdominal irradiation.
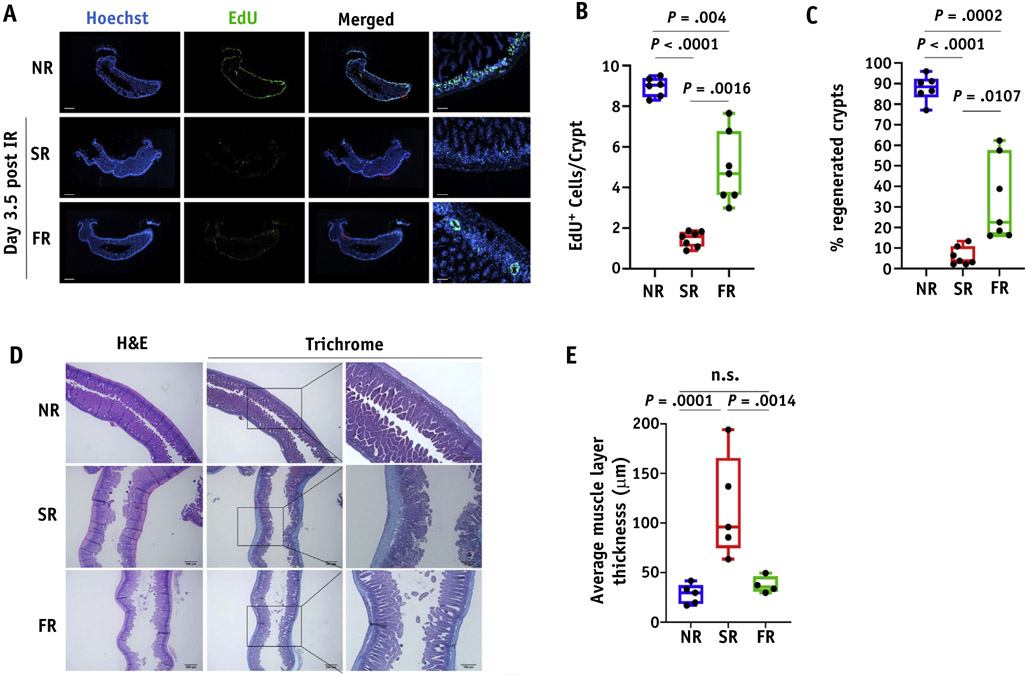
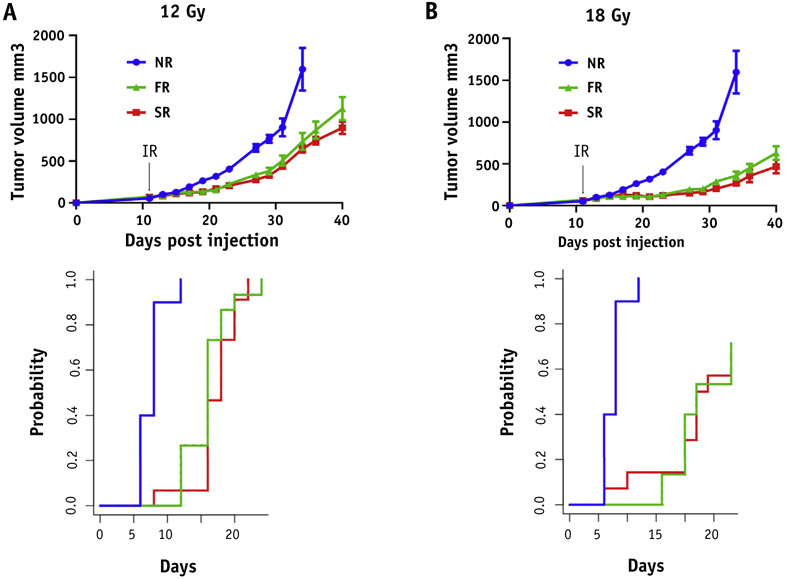
Results: The double scattering and collimation apparatus was dosimetrically validated with dose rates of 78 ± 9 Gy per second and 0.9 ± 0.08 Gy per second for the FLASH and standard PRT. Whole abdominal FLASH PRT at 15 Gy significantly reduced the loss of proliferating cells in intestinal crypts compared with standard PRT. Studies with local intestinal irradiation at 18 Gy revealed a reduction to near baseline levels of intestinal fibrosis for FLASH-PRT compared with standard PRT. Despite this difference, FLASH-PRT did not demonstrate tumor radioprotection in MH641905 pancreatic cancer flank tumors after 12 or 18 Gy irradiation.
Conclusions: We have designed and dosimetrically validated a FLASH-PRT system with accurate control of beam flux on a millisecond time scale and online monitoring of the integral and dose delivery time structure. Using this system, we found that FLASH-PRT decreases acute cell loss and late fibrosis after whole-abdomen and focal intestinal RT, whereas tumor growth inhibition is preserved between the 2 modalities.
Copyright © 2019 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Favaudon V, Caplier L, Monceau V, et al. Ultrahigh dose-rate FLASH irradiation increases the differential response between normal and tumor tissue in mice. Sci Transl Med 2014;6:245ra93. - PubMed
-
- Harrington KJ. Ultrahigh dose-rate radiotherapy: Next steps for FLASH-RT. Clin Cancer Res 2019;25:3–5. - PubMed
-
- Vozenin MC, De Fornel P, Petersson K, et al. The advantage of FLASH radiotherapy confirmed in mini-pig and cat-cancer patients. Clin Cancer Res 2019;25:35–42. - PubMed
-
- Schmid TE, Dollinger G, Hauptner A, et al. No evidence for a different rbe between pulsed and continuous 20 mev protons. Radiat Res 2009;172:567–574. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
