

Modifiable risk factors for carotid atherosclerosis: a meta-analysis and systematic review
- PMID: 31930033
- PMCID: PMC6944535
- DOI: 10.21037/atm.2019.10.115
Modifiable risk factors for carotid atherosclerosis: a meta-analysis and systematic review
Abstract
Background: Carotid atherosclerosis is a major cause of stroke, but the conclusion about risk factors for carotid atherosclerosis is still controversial. The aim of our present meta-analysis and systematic review was to explore the modifiable risk factors for carotid atherosclerosis.
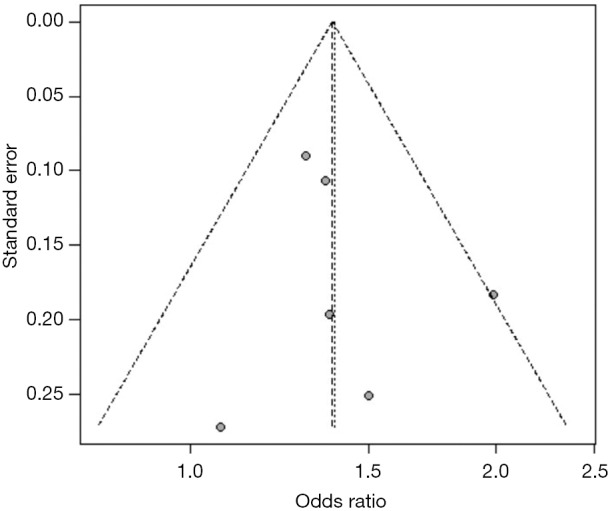
Methods: We searched PubMed from January 1962 to October 2018 to include longitudinal and cross-sectional studies. The results were pooled using random effects model. Heterogeneity was measured by I2 statistic and publication bias was assessed by funnel plots.
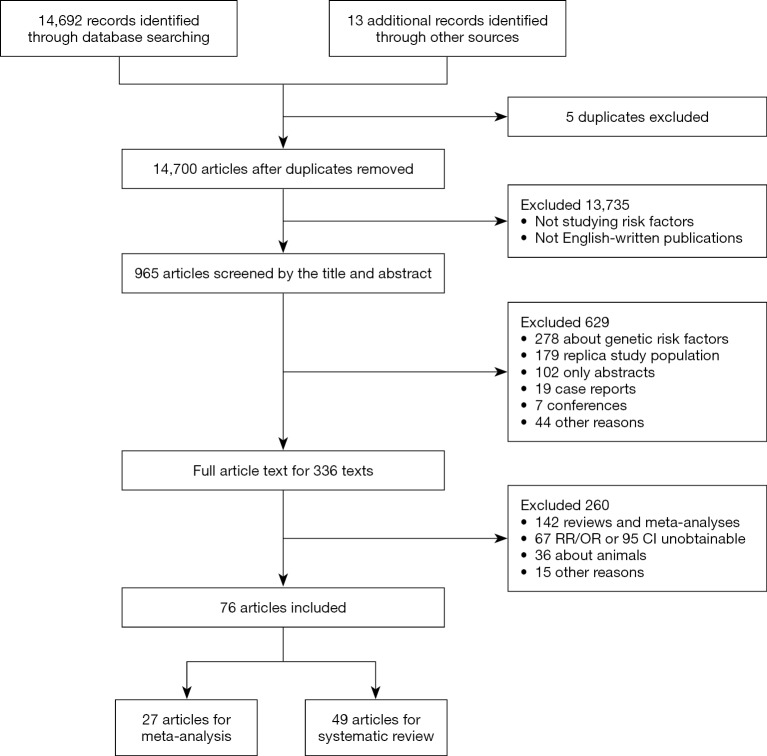
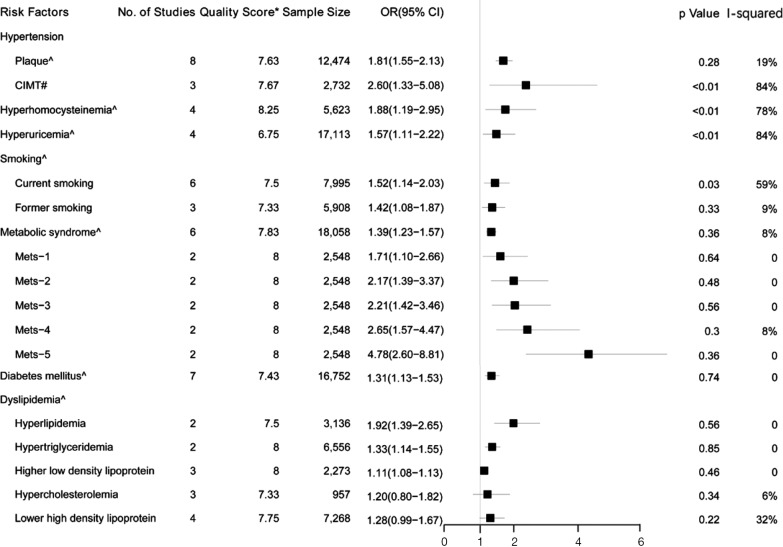
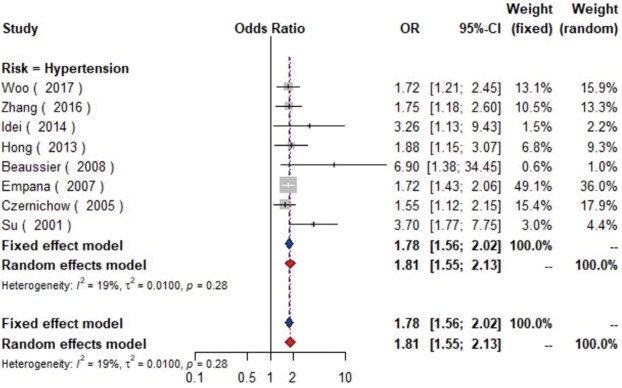
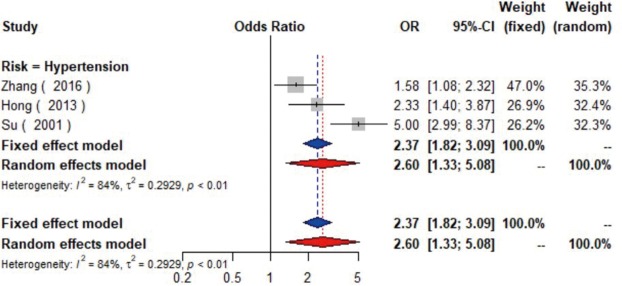
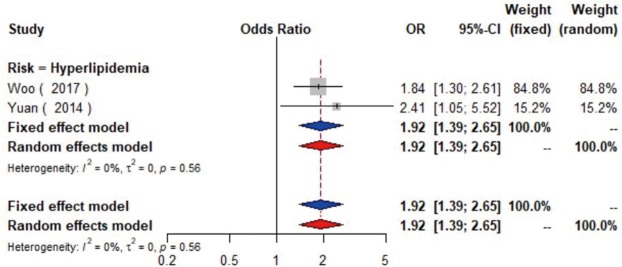
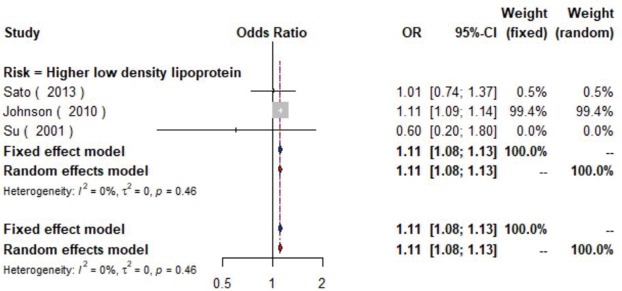
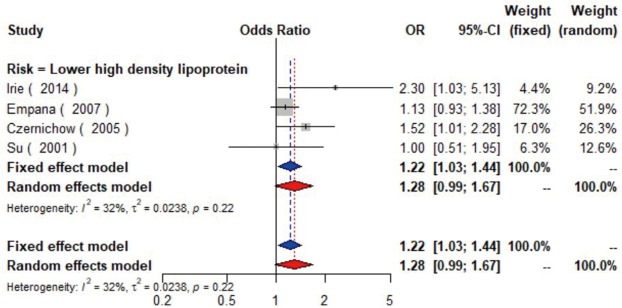
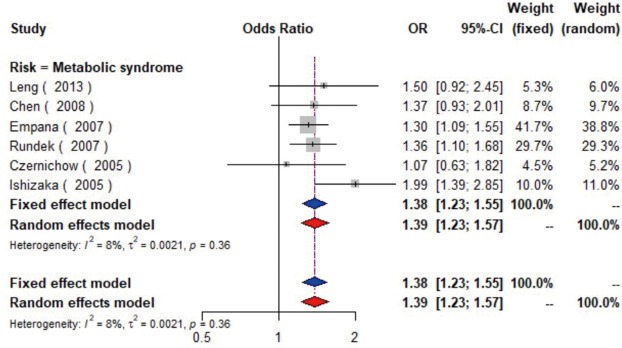
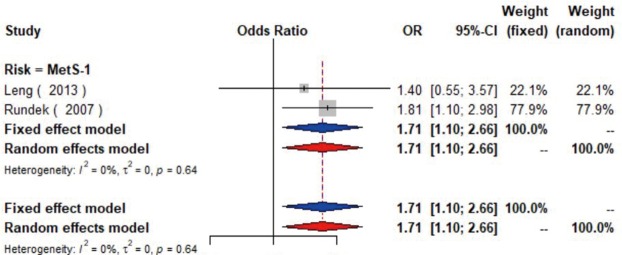
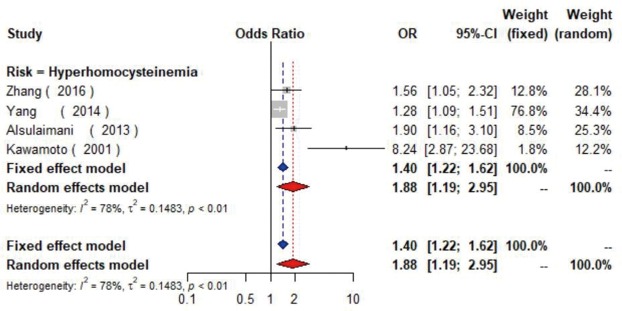
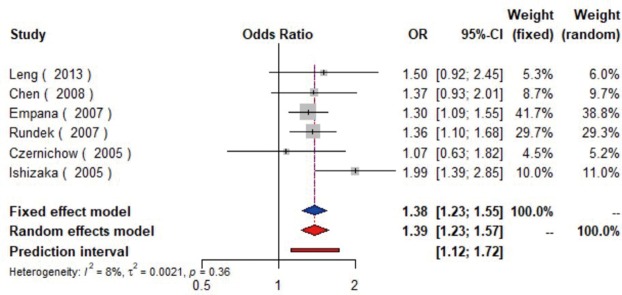
Results: A total of 14,700 articles were screened, of which 76 with 27 factors were eligible. Our meta-analysis of cross-sectional studies indicated nine factors (hyperlipidemia, hyperhomocysteinemia, hypertension, hyperuricemia, smoking, metabolic syndrome, hypertriglyceridemia, diabetes, and higher low density lipoprotein) were significantly associated with the presence of carotid plaque, among which four (hyperlipidemia, hyperhomocysteinemia, hypertension, and hyperuricemia) could elevate the risk of atherosclerosis by at least 50%; and one factor (hypertension) was associated with increased carotid intima-media thickness. In the systematic review, another five factors [negative emotion, socioeconomic strain, alcohol, air pollution, and obstructive sleep apnea syndrome (OSAS)] were also related to the presence of atherosclerosis. The cross-sectional associations with most of the above 14 factors were further confirmed by longitudinal studies. Among them, the managements of 4 factors (hypertension, hyperlipidemia, diabetes and OSAS) were indicated to prevent carotid atherosclerosis by cohort studies.
Conclusions: Effective interventions targeting pre-existing disease, negative emotion, lifestyle and diet may reduce the risk of carotid atherosclerosis. Further good-quality prospective studies are needed to confirm these findings.
Keywords: Carotid atherosclerosis; carotid intima-media thickness; carotid plaque; meta-analysis; risk factors.
2019 Annals of Translational Medicine. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures

















References
LinkOut - more resources
Full Text Sources
Medical