

Hybrid computed tomography and magnetic resonance imaging 3D printed models for neurosurgery planning
- PMID: 31930085
- PMCID: PMC6944557
- DOI: 10.21037/atm.2019.10.109
Hybrid computed tomography and magnetic resonance imaging 3D printed models for neurosurgery planning
Abstract
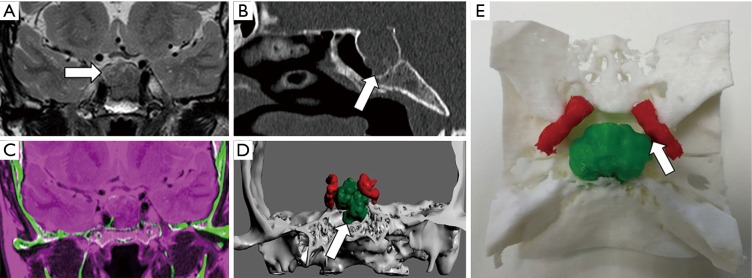
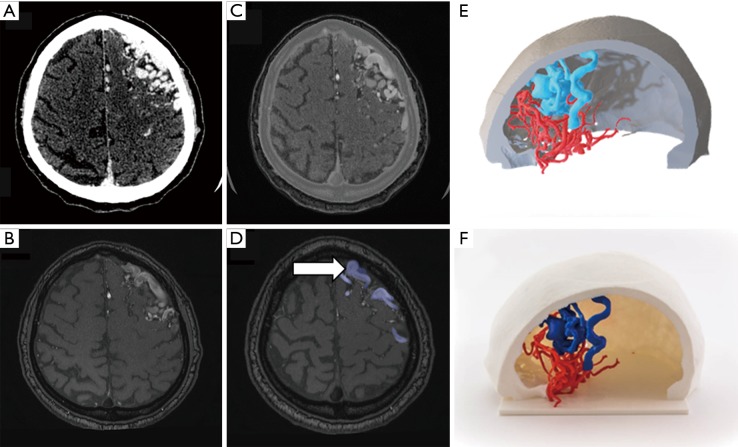
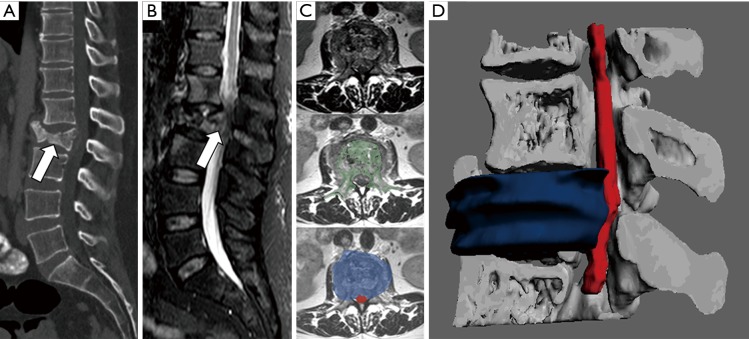
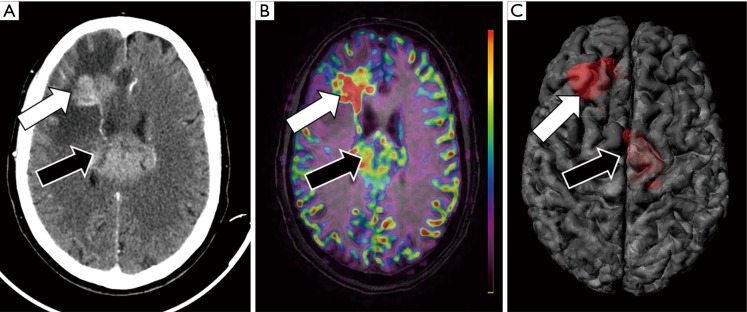
In the last decade, the clinical applications of three-dimensional (3D) printed models, in the neurosurgery field among others, have expanded widely based on several technical improvements in 3D printers, an increased variety of materials, but especially in postprocessing software. More commonly, physical models are obtained from a unique imaging technique with potential utilization in presurgical planning, generation/creation of patient-specific surgical material and personalized prosthesis or implants. Using specific software solutions, it is possible to obtain a more accurate segmentation of different anatomical and pathological structures and a more precise registration between different medical image sources allowing generating hybrid computed tomography (CT) and magnetic resonance imaging (MRI) 3D printed models. The need of neurosurgeons for a better understanding of the complex anatomy of central nervous system (CNS) and spine is pushing the use of these hybrid models, which are able to combine morphological information from CT and MRI, and also able to add physiological data from advanced MRI sequences, such as diffusion-weighted imaging (DWI), diffusion tensor imaging (DTI), perfusion weighted imaging (PWI) and functional MRI (fMRI). The inclusion of physiopathological data from advanced MRI sequences enables neurosurgeons to identify those areas with increased biological aggressiveness within a certain lesion prior to surgery or biopsy procedures. Preliminary data support the use of this more accurate presurgical perspective, to select the better surgical approach, reduce the global length of surgery and minimize the rate of intraoperative complications, morbidities or patient recovery times after surgery. The use of 3D printed models in neurosurgery has also demonstrated to be a valid tool for surgeons training and to improve communication between specialists and patients. Further studies are needed to test the feasibility of this novel approach in common clinical practice and determine the degree of improvement the neurosurgeons receive and the potential impact on patient outcome.
Keywords: Three-dimensional printing (3D printing); brain; computed tomography (CT); hybrid imaging; magnetic resonance imaging (MRI); neurosurgery; spine.
2019 Annals of Translational Medicine. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
-
- Waran V, Pancharatnam D, Thambinayagam HC, et al. The utilization of cranial models created using rapid prototyping techniques in the development of models for navigation training. J Neurol Surg A Cent Eur Neurosurg 2014;75:12-5. - PubMed