

Assessment of the Validity of the 2HELPS2B Score for Inpatient Seizure Risk Prediction
- PMID: 31930362
- PMCID: PMC6990873
- DOI: 10.1001/jamaneurol.2019.4656
Assessment of the Validity of the 2HELPS2B Score for Inpatient Seizure Risk Prediction
Erratum in
-
Error in Author's Name.JAMA Neurol. 2020 Apr 1;77(4):527. doi: 10.1001/jamaneurol.2020.0140. JAMA Neurol. 2020. PMID: 32091539 Free PMC article. No abstract available.
Abstract
Importance: Seizure risk stratification is needed to boost inpatient seizure detection and to improve continuous electroencephalogram (cEEG) cost-effectiveness. 2HELPS2B can address this need but requires validation.
Objective: To use an independent cohort to validate the 2HELPS2B score and develop a practical guide for its use.
Design, setting, and participants: This multicenter retrospective medical record review analyzed clinical and EEG data from patients 18 years or older with a clinical indication for cEEG and an EEG duration of 12 hours or longer who were receiving consecutive cEEG at 6 centers from January 2012 to January 2019. 2HELPS2B was evaluated with the validation cohort using the mean calibration error (CAL), a measure of the difference between prediction and actual results. A Kaplan-Meier survival analysis was used to determine the duration of EEG monitoring to achieve a seizure risk of less than 5% based on the 2HELPS2B score calculated on first- hour (screening) EEG. Participants undergoing elective epilepsy monitoring and those who had experienced cardiac arrest were excluded. No participants who met the inclusion criteria were excluded.
Main outcomes and measures: The main outcome was a CAL error of less than 5% in the validation cohort.
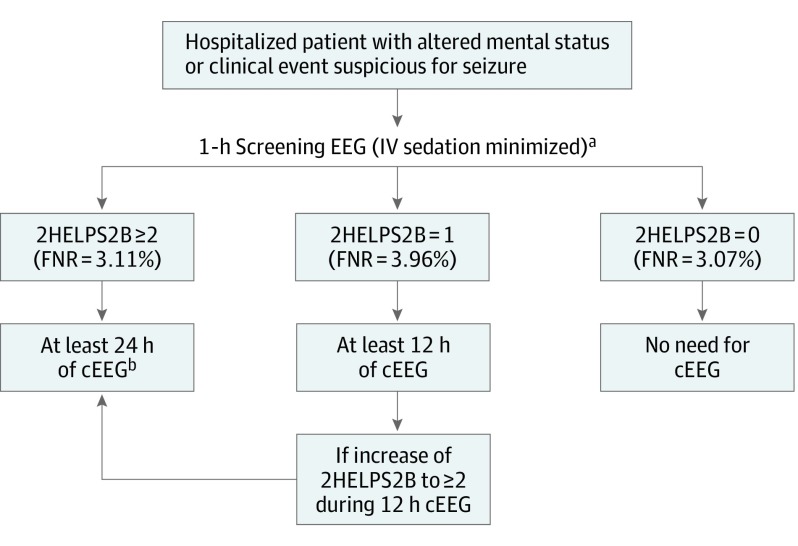
Results: The study included 2111 participants (median age, 51 years; 1113 men [52.7%]; median EEG duration, 48 hours) and the primary outcome was met with a validation cohort CAL error of 4.0% compared with a CAL of 2.7% in the foundational cohort (P = .13). For the 2HELPS2B score calculated on only the first hour of EEG in those without seizures during that hour, the CAL error remained at less than 5.0% at 4.2% and allowed for stratifying patients into low- (2HELPS2B = 0; <5% risk of seizures), medium- (2HELPS2B = 1; 12% risk of seizures), and high-risk (2HELPS2B, ≥2; risk of seizures, >25%) groups. Each of the categories had an associated minimum recommended duration of EEG monitoring to achieve at least a less than 5% risk of seizures, a 2HELPS2B score of 0 at 1-hour screening EEG, a 2HELPS2B score of 1 at 12 hours, and a 2HELPS2B score of 2 or greater at 24 hours.
Conclusions and relevance: In this study, 2HELPS2B was validated as a clinical tool to aid in seizure detection, clinical communication, and cEEG use in hospitalized patients. In patients without prior clinical seizures, a screening 1-hour EEG that showed no epileptiform findings was an adequate screen. In patients with any highly epileptiform EEG patterns during the first hour of EEG (ie, a 2HELPS2B score of ≥2), at least 24 hours of recording is recommended.
Conflict of interest statement
Figures



References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
