

Mapping the ischemic penumbra and predicting stroke progression in acute ischemic stroke: the overlooked role of susceptibility weighted imaging
- PMID: 31930428
- PMCID: PMC6955386
- DOI: 10.1186/s13244-019-0810-y
Mapping the ischemic penumbra and predicting stroke progression in acute ischemic stroke: the overlooked role of susceptibility weighted imaging
Abstract
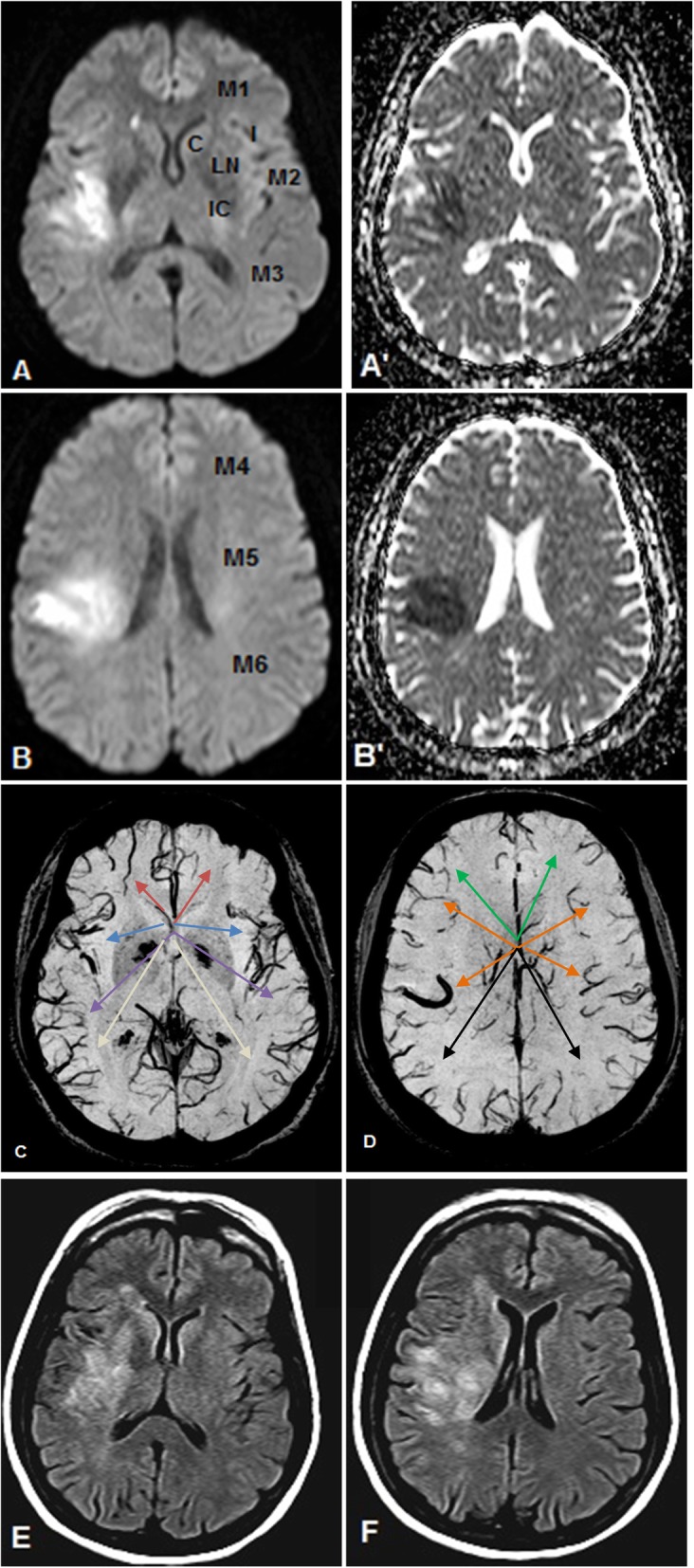
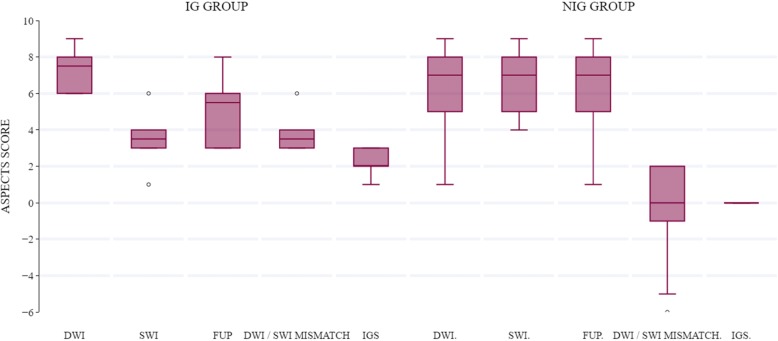
Objectives: Asymmetrically prominent veins (APVs) detected on susceptibility weighted imaging (SWI) in acute stroke patients are assumed to signify compromised cerebral perfusion. We aimed to explore the role of APVs in identifying the ischemic penumbra and predicting stroke progression in acute stroke patients METHODS: Twenty patients with a middle cerebral artery ischemic infarction presenting within 24 h of symptoms onset underwent SWI following our standard MR stroke protocol imaging sequences which included diffusion-weighted imaging (DWI). Follow-up (FUP) FLAIR images were obtained at least 5 days after the initial MRI study. The Alberta Stroke Program Early CT Score (ASPECTS) was used to determine the initial infarct size, extent of APVs and final infarct size on initial DWI, SWI, and FUP images respectively. For each patient, SWI was compared with DWI images to determine match/mismatch of their respective ASPECTS values and calculate mismatch scores, whereas acute DWI findings were compared with follow-up images to identify infarct growth (IG) and calculate infarction growth scores (IGS).
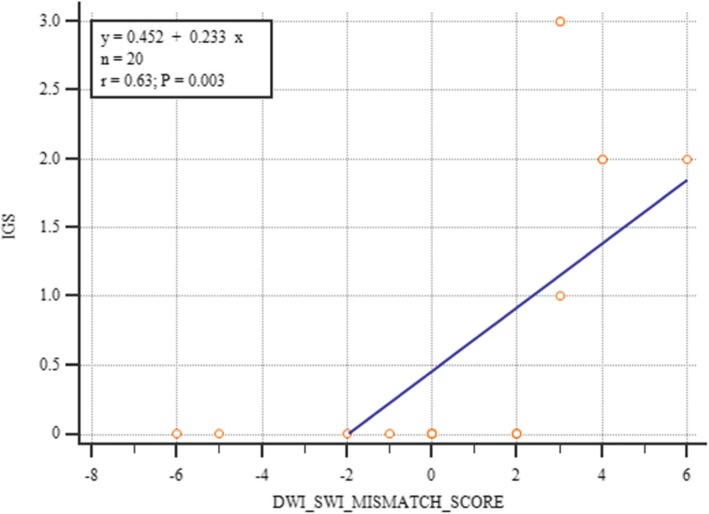
Results: IG occurred in 6/10 patients with a positive DWI-SWI mismatch and in none of the patients without a positive DWI-SWI mismatch. A positive DWI/SWI mismatch was significantly associated with IG (χ2 = 8.57, p = 0.0138, Cramer's V = 0.65). A significant inverse correlation was found between SWI ASPECTS and IGS (rs = - 0.702, p = 0.001). DWI-SWI mismatch scores were strongly correlated with IGS. (rs = 0.788, p = 0.000) CONCLUSION: A positive DWI-SWI mismatch is an indicator of the ischemic penumbra and a predictor of infarct expansion if left untreated.
Keywords: Asymmetrically prominent veins; DWI-SWI mismatch; Penumbra; Stroke; Susceptibility weighted imaging.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Tomandl BF, Klotz E, Handschu R, et al. Comprehensive imaging of ischemic stroke with multisection CT. Radiographics. 2003;23:565–592. - PubMed
-
- Munich SA, Shakir HJ, Snyder KV. Role of CT perfusion in acute stroke management. Cor et Vasa. 2016;58(2):e215–e224.
-
- Kao Hung-Wen, Tsai Fong Y., Hasso Anton N. Predicting stroke evolution: comparison of susceptibility-weighted MR imaging with MR perfusion. European Radiology. 2012;22(7):1397–1403. - PubMed
LinkOut - more resources
Full Text Sources
