

Tracking Cardiac Rehabilitation Participation and Completion Among Medicare Beneficiaries to Inform the Efforts of a National Initiative
- PMID: 31931615
- PMCID: PMC8091573
- DOI: 10.1161/CIRCOUTCOMES.119.005902
Tracking Cardiac Rehabilitation Participation and Completion Among Medicare Beneficiaries to Inform the Efforts of a National Initiative
Abstract
Background: Despite cardiac rehabilitation (CR) being shown to improve health outcomes among patients with heart disease, its use has been suboptimal. In response, the Million Hearts Cardiac Rehabilitation Collaborative developed a road map to improve CR use, including increasing participation rates to ≥70% by 2022. This observational study provides current estimates to measure progress and identifies the populations and regions most at risk for CR service underutilization.
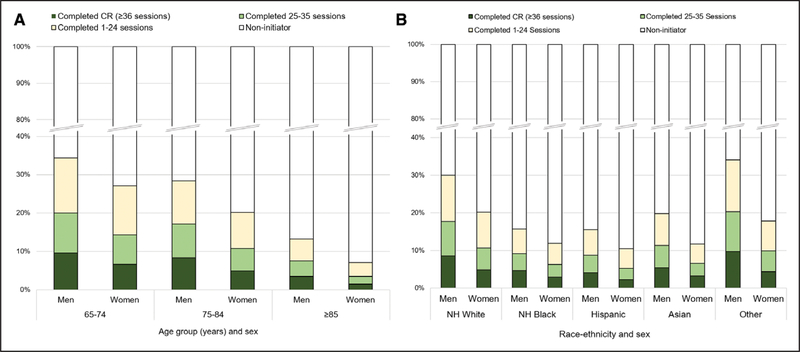
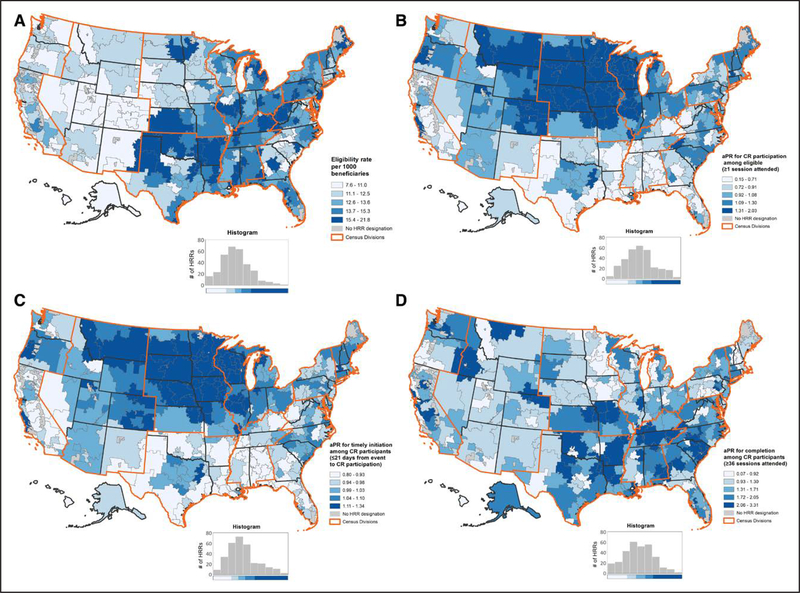
Methods and results: We identified Medicare fee-for-service beneficiaries who were CR eligible in 2016, and assessed CR participation (≥1 CR session attended), timely initiation (participation within 21 days of event), and completion (≥36 sessions attended) through 2017. Measures were assessed overall, by beneficiary characteristics and geography, and by primary CR-qualifying event type (acute myocardial infarction hospitalization; coronary artery bypass surgery; heart valve repair/replacement; percutaneous coronary intervention; or heart/heart-lung transplant). Among 366 103 CR-eligible beneficiaries, 89 327 (24.4%) participated in CR, of whom 24.3% initiated within 21 days and 26.9% completed CR. Eligibility was highest in the East South Central Census Division (14.8 per 1000). Participation decreased with increasing age, was lower among women (18.9%) compared with men (28.6%; adjusted prevalence ratio: 0.91 [95% CI, 0.90-0.93]) was lower among Hispanics (13.2%) and non-Hispanic blacks (13.6%) compared with non-Hispanic whites (25.8%; adjusted prevalence ratio: 0.63 [0.61-0.66] and 0.70 [0.67-0.72], respectively), and varied by hospital referral region and Census Division (range: 18.6% [East South Central] to 39.1% [West North Central]) and by qualifying event type (range: 7.1% [acute myocardial infarction without procedure] to 55.3% [coronary artery bypass surgery only]). Timely initiation varied by geography and qualifying event type; completion varied by geography.
Conclusions: Only 1 in 4 CR-eligible Medicare beneficiaries participated in CR and marked disparities were observed. Reinforcement of current effective strategies and development of new strategies will be critical to address the noted disparities and achieve the 70% participation goal.
Keywords: cardiac rehabilitation; coronary artery bypass; heart diseases; myocardial infarction; percutaneous coronary intervention.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
