

Cardiac Intervention Improves Heart Disease and Clinical Outcomes in Patients With Muscular Dystrophy in a Multidisciplinary Care Setting
- PMID: 31931688
- PMCID: PMC7033817
- DOI: 10.1161/JAHA.119.014004
Cardiac Intervention Improves Heart Disease and Clinical Outcomes in Patients With Muscular Dystrophy in a Multidisciplinary Care Setting
Abstract
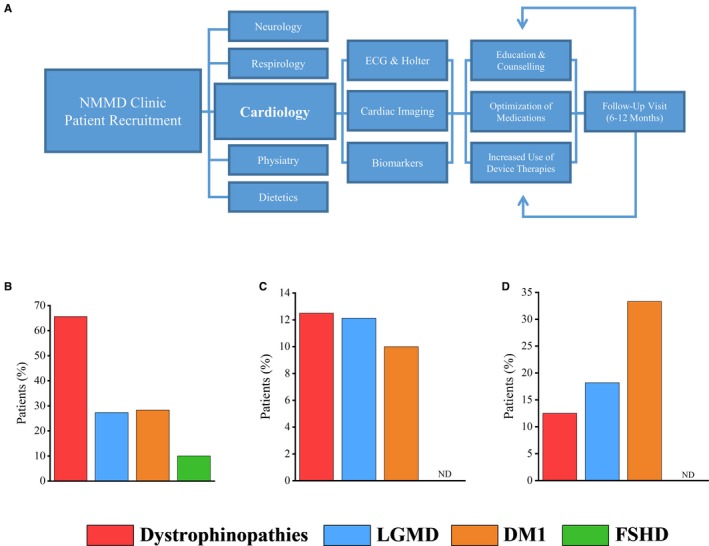
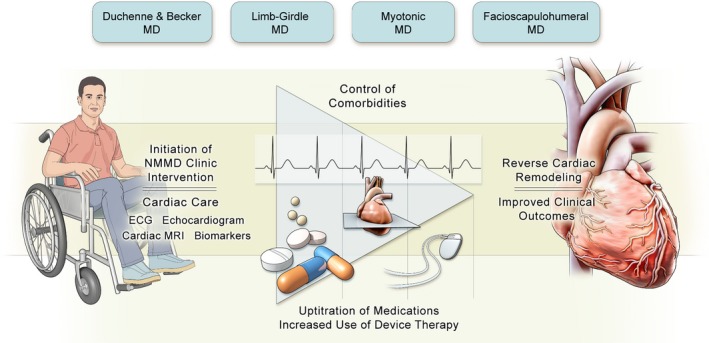
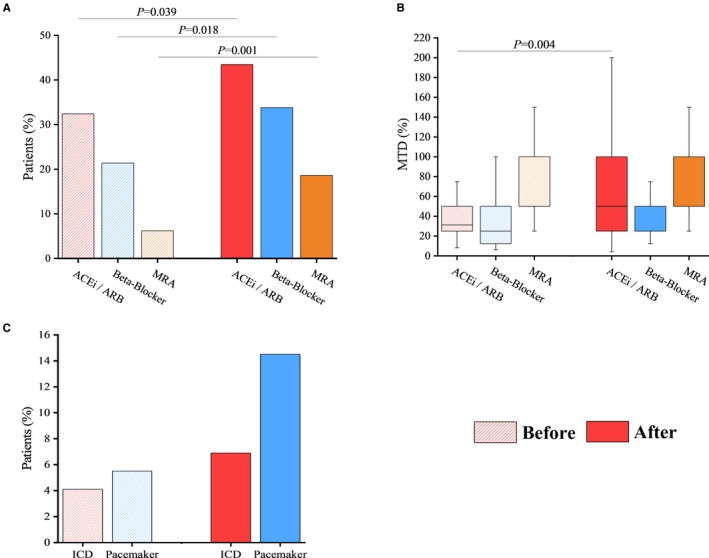
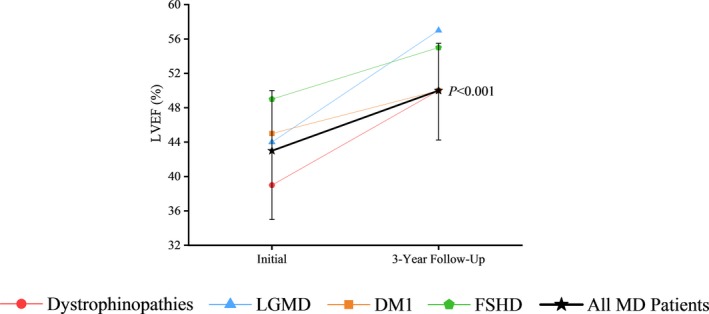
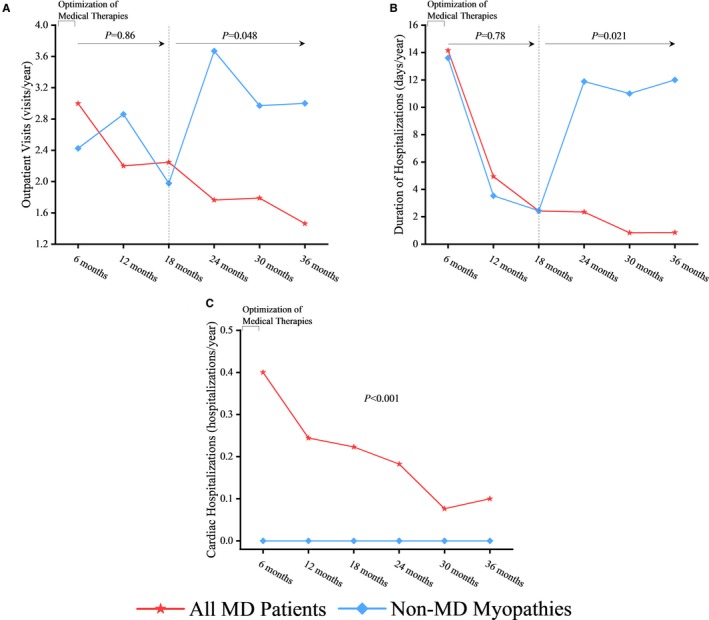
Background Patients with muscular dystrophy (MD) represent a vulnerable patient population with no clearly defined care model in modern-day clinical practice to manage a high burden of heart disease and comorbidities. We demonstrate the effectiveness of cardiac interventions, namely the initiation and optimization of medical and device therapies, as part of a multidisciplinary care approach to improve clinical outcomes in patients with MD. Methods and Results We conducted a prospective cohort study at the Neuromuscular Multidisciplinary clinic following patients with dystrophinopathies, limb-girdle MD, type 1 myotonic dystrophy, and facioscapulohumeral MD. A negative control group classified as non-MD myopathies without heart disease, was also tracked. Our cohort of 185 patients (median age: 42 years; 79 [42.7%] women), included 145 patients with MD. Cardiomyopathy was present in 65.6% of the patients with dystrophinopathies (21 of 32) and 27.3% of the patients with limb-girdle MD (9 of 33). Conduction abnormalities were common in type 1 myotonic dystrophy (33.3% [20/60] patients). Cardiac intervention reversed systolic dysfunction, with left ventricular ejection fraction improving from 43% to 50.0% over a 3-year period. A sustained reduction in healthcare utilization was also observed. The number of outpatient clinic visits decreased from 3.0 to 1.5 visits per year, the duration of hospitalizations was reduced from 14.2 to 0.9 days per year, and the number of cardiac-related hospitalizations decreased from 0.4 to 0.1 hospitalizations per year associated with low mortality. Conclusions Our study demonstrates that cardiac intervention as part of a comprehensive multidisciplinary care approach to treating patients with MD leads to a sustained improvement in clinical outcomes.
Keywords: heart disease; medical therapy; multidisciplinary care; muscular dystrophy; outcome data.
Figures
References
-
- Koeks Z, Bladen CL, Salgado D, van Zwet E, Pogoryelova O, McMacken G, Monges S, Foncuberta ME, Kekou K, Kosma K, Dawkins H, Lamont L, Bellgard MI, Roy AJ, Chamova T, Guergueltcheva V, Chan S, Korngut L, Campbell C, Dai Y, Wang J, Barisic N, Brabec P, Lahdetie J, Walter MC, Schreiber‐Katz O, Karcagi V, Garami M, Herczegfalvi A, Viswanathan V, Bayat F, Buccella F, Ferlini A, Kimura E, van den Bergen JC, Rodrigues M, Roxburgh R, Lusakowska A, Kostera‐Pruszczyk A, Santos R, Neagu E, Artemieva S, Rasic VM, Vojinovic D, Posada M, Bloetzer C, Klein A, Diaz‐Manera J, Gallardo E, Karaduman AA, Oznur T, Topaloglu H, El Sherif R, Stringer A, Shatillo AV, Martin AS, Peay HL, Kirschner J, Flanigan KM, Straub V, Bushby K, Beroud C, Verschuuren JJ, Lochmuller H. Clinical outcomes in Duchenne muscular dystrophy: a study of 5345 patients from the TREAT‐NMD DMD global database. J Neuromuscul Dis. 2017;4:293–306. - PMC - PubMed
-
- Bushby K, Finkel R, Birnkrant DJ, Case LE, Clemens PR, Cripe L, Kaul A, Kinnett K, McDonald C, Pandya S, Poysky J, Shapiro F, Tomezsko J, Constantin C; Group DMDCCW . Diagnosis and management of Duchenne muscular dystrophy, part 2: implementation of multidisciplinary care. Lancet Neurol. 2010;9:177–189. - PubMed
-
- Arbustini E, Di Toro A, Giuliani L, Favalli V, Narula N, Grasso M. Cardiac phenotypes in hereditary muscle disorders. J Am Coll Cardiol. 2018;72:2485–2506. - PubMed
-
- Miskew Nichols B, Nikhanj A, Wang F, Freed DH, Oudit GY. Advanced dilated cardiomyopathy in a patient with Hutterite limb‐girdle muscular dystrophy: use of a left ventricular assist device. Circ Heart Fail. 2018;11:e004960. - PubMed
-
- Silva MC, Meira ZM, Gurgel Giannetti J, da Silva MM, Campos AF, Barbosa Mde M, Starling Filho GM, Ferreira Rde A, Zatz M, Rochitte CE. Myocardial delayed enhancement by magnetic resonance imaging in patients with muscular dystrophy. J Am Coll Cardiol. 2007;49:1874–1879. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
