

Translational research of temporomandibular joint pathology: a preliminary biomarker and fMRI study
- PMID: 31931814
- PMCID: PMC6956559
- DOI: 10.1186/s12967-019-02202-0
Translational research of temporomandibular joint pathology: a preliminary biomarker and fMRI study
Abstract
Background: The temporomandibular joint (TMJ) is well innervated by braches of the trigeminal nerve. The temporomandibular joint disorders (TMD) can cause neural-inflammation in the peripheral nervous system (PNS) at the site of injury, or compression, and may have systemic effects on the central nervous system (CNS). Neural-inflammation causes elevations in cytokine expression and microglia activation. When the site of injury, or compression is treated, or relieved, neural inflammation is reduced. These changes can be seen and measured with fMRI brain activities.
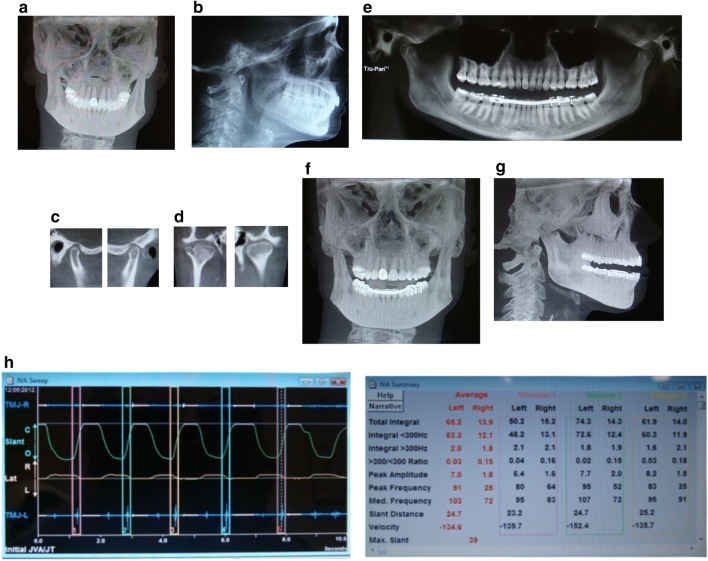
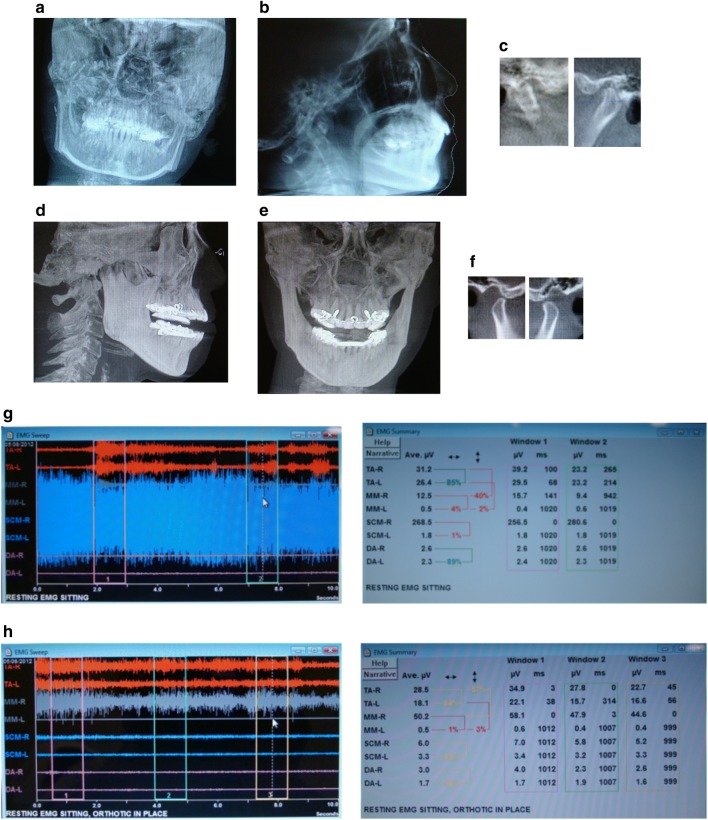
Methods: For this study, patients with comorbid TMD and systemic/neurologic conditions were compared using clinical diagnostic markers, inflammatory, pain, tissue destruction enzymatic biomarkers, and functional magnetic resonance imaging (fMRI) activity of the brain, with and without a custom-made dental orthotic.
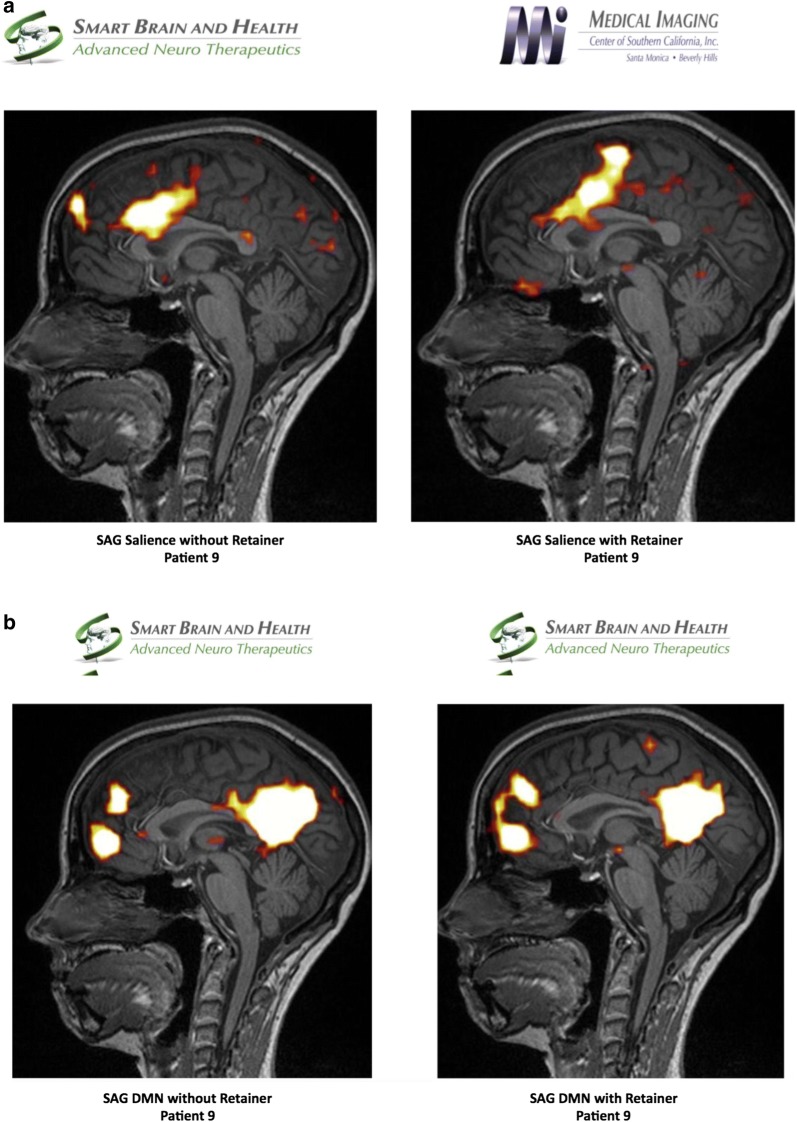
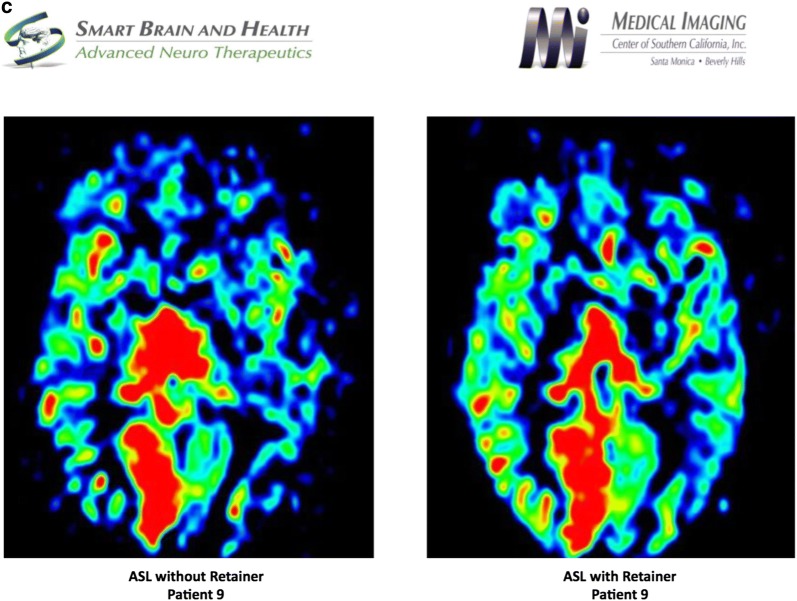
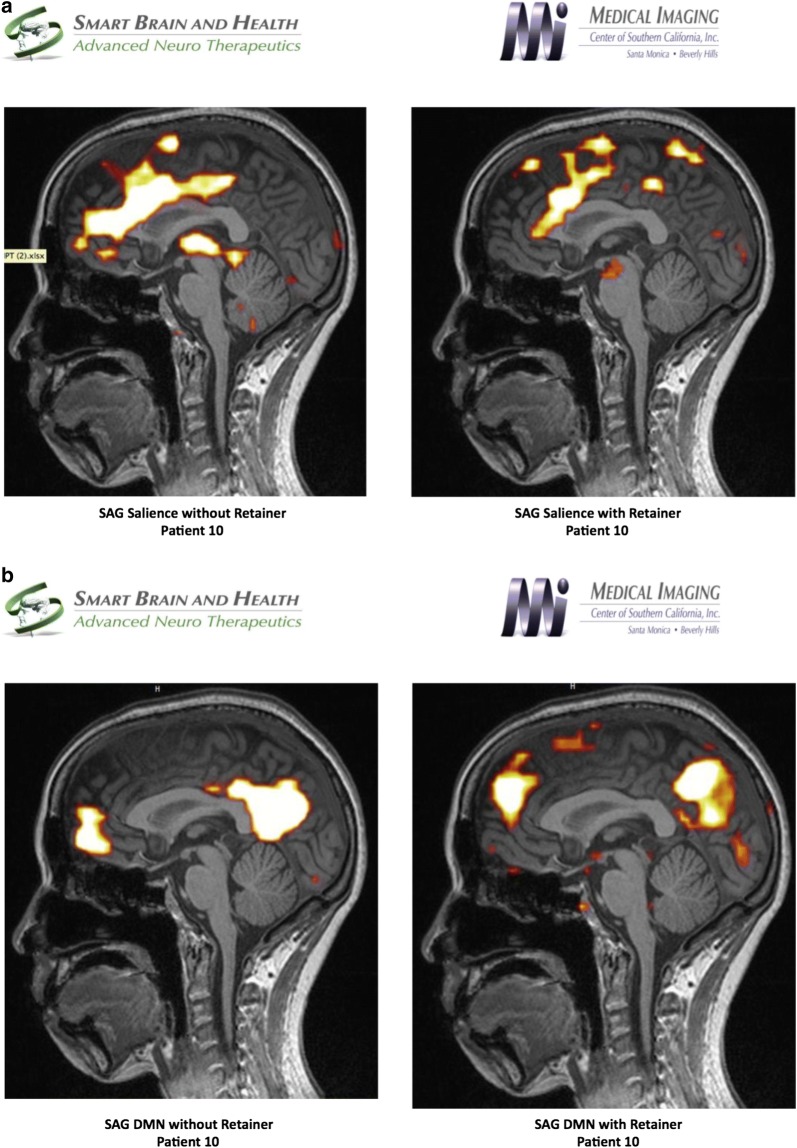
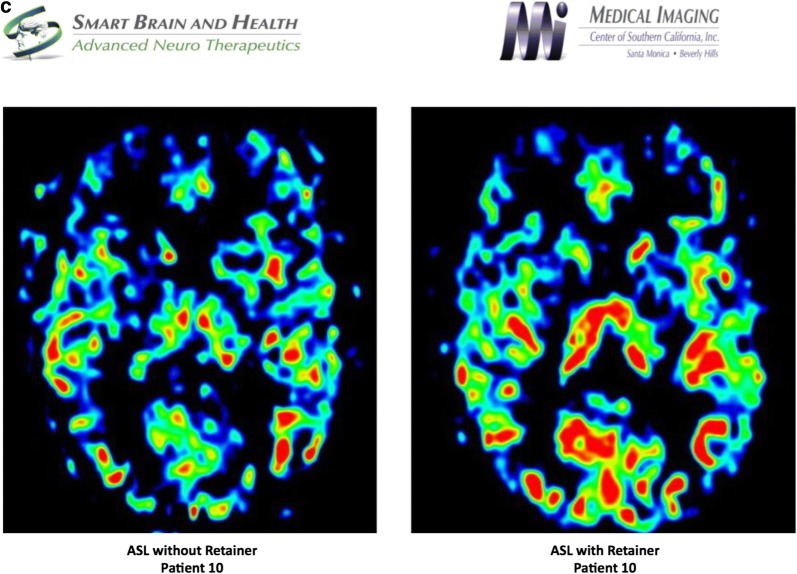
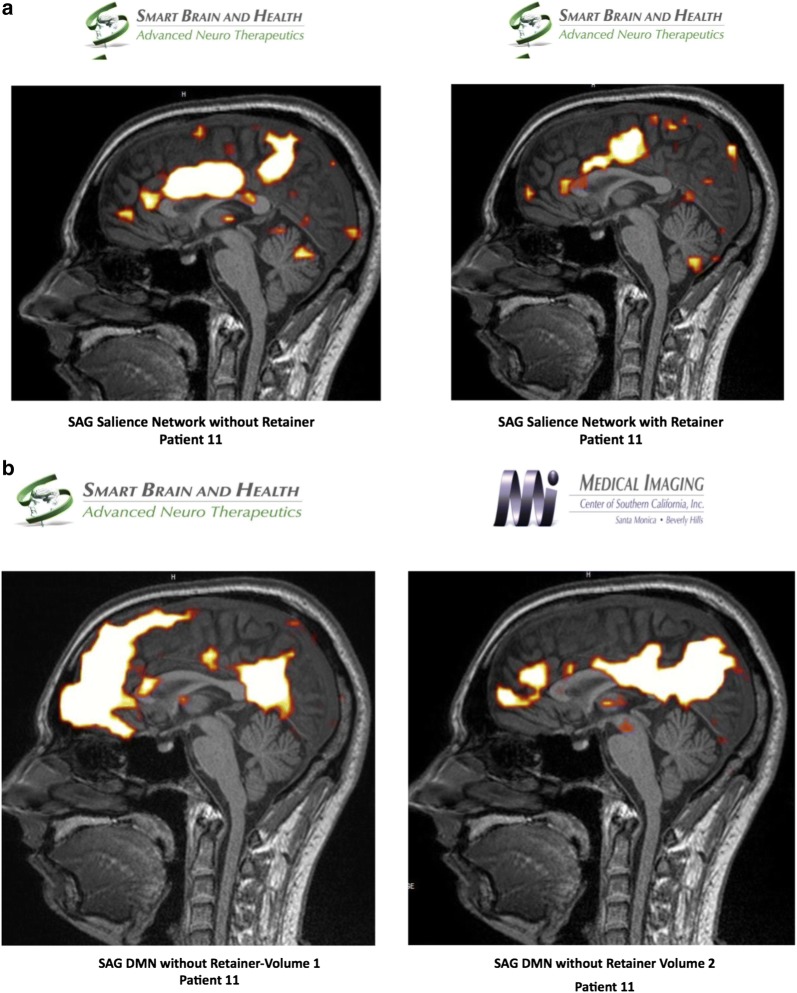
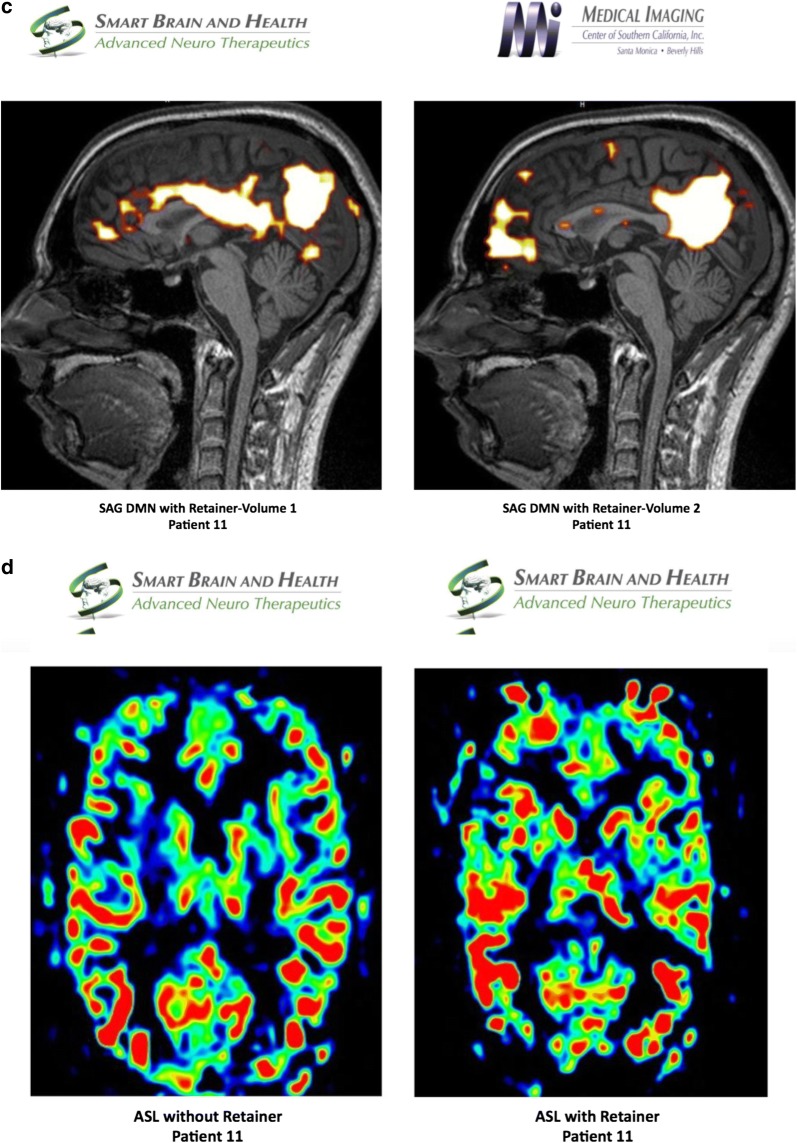
Results: Our results showed a correlation between the clinical diagnosis of the pathological TMJ, biomarkers and the fMRI study. There was a marked elevation of biomarkers in samples taken from TMJ of patients who were clinically diagnosed with TMD. The fMRI study of TMD patients showed an abnormal hyper-connected salience network and a diminished blood flow to the anterior frontal lobes when they did not wear their customized dental orthotics.
Conclusions: Our findings highlight the importance of TMJ-CNS connections and use of fMRI as an investigative tool for understanding TMD and its related neurological pathologies.
Keywords: Arterial spin labeling (ASL); Blood oxygenation level dependent (BOLD); Default mode network (DMN); Dental orthotic; Fractional anisotropy (FA); Functional magnetic resonance imaging (fMRI); Microglia cells; Temporomandibular joint (TMJ); Temporomandibular joint disorders (TMD); Trigeminal ganglion (TG).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- De Leeuw R, Klasser GD, Albuquerque RJ. Are female patients with orofacial pain medically compromised? JADA. 2005;136(4):459–468. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
