

Should the ultrasound probe replace your stethoscope? A SICS-I sub-study comparing lung ultrasound and pulmonary auscultation in the critically ill
- PMID: 31931844
- PMCID: PMC6958607
- DOI: 10.1186/s13054-019-2719-8
Should the ultrasound probe replace your stethoscope? A SICS-I sub-study comparing lung ultrasound and pulmonary auscultation in the critically ill
Abstract
Background: In critically ill patients, auscultation might be challenging as dorsal lung fields are difficult to reach in supine-positioned patients, and the environment is often noisy. In recent years, clinicians have started to consider lung ultrasound as a useful diagnostic tool for a variety of pulmonary pathologies, including pulmonary edema. The aim of this study was to compare lung ultrasound and pulmonary auscultation for detecting pulmonary edema in critically ill patients.
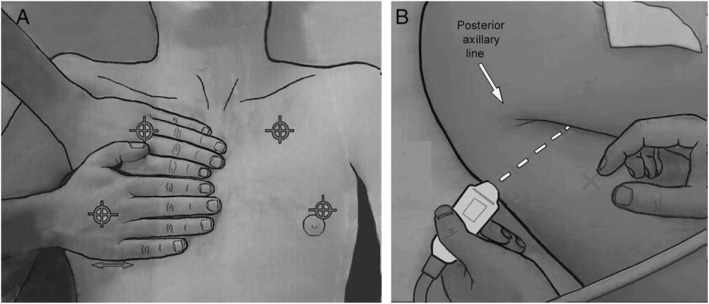
Methods: This study was a planned sub-study of the Simple Intensive Care Studies-I, a single-center, prospective observational study. All acutely admitted patients who were 18 years and older with an expected ICU stay of at least 24 h were eligible for inclusion. All patients underwent clinical examination combined with lung ultrasound, conducted by researchers not involved in patient care. Clinical examination included auscultation of the bilateral regions for crepitations and rhonchi. Lung ultrasound was conducted according to the Bedside Lung Ultrasound in Emergency protocol. Pulmonary edema was defined as three or more B lines in at least two (bilateral) scan sites. An agreement was described by using the Cohen κ coefficient, sensitivity, specificity, negative predictive value, positive predictive value, and overall accuracy. Subgroup analysis were performed in patients who were not mechanically ventilated.
Results: The Simple Intensive Care Studies-I cohort included 1075 patients, of whom 926 (86%) were eligible for inclusion in this analysis. Three hundred seven of the 926 patients (33%) fulfilled the criteria for pulmonary edema on lung ultrasound. In 156 (51%) of these patients, auscultation was normal. A total of 302 patients (32%) had audible crepitations or rhonchi upon auscultation. From 130 patients with crepitations, 86 patients (66%) had pulmonary edema on lung ultrasound, and from 209 patients with rhonchi, 96 patients (46%) had pulmonary edema on lung ultrasound. The agreement between auscultation findings and lung ultrasound diagnosis was poor (κ statistic 0.25). Subgroup analysis showed that the diagnostic accuracy of auscultation was better in non-ventilated than in ventilated patients.
Conclusion: The agreement between lung ultrasound and auscultation is poor.
Trial registration: NCT02912624. Registered on September 23, 2016.
Keywords: Auscultation; Clinical examination; Critical care; Diagnostic accuracy; Lung ultrasound; Prospective study; Pulmonary edema.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Shrestha GS, Weeratunga D, Baker K. Point-of-care lung ultrasound in critically ill patients. Rev Recent Clin Trials. 2018;13:15–26. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
