

Infectious morbidity of breastfed, HIV-exposed uninfected infants under conditions of universal antiretroviral therapy in South Africa: a prospective cohort study
- PMID: 31932246
- PMCID: PMC7235356
- DOI: 10.1016/S2352-4642(19)30375-X
Infectious morbidity of breastfed, HIV-exposed uninfected infants under conditions of universal antiretroviral therapy in South Africa: a prospective cohort study
Abstract
Background: Without breastfeeding and maternal antiretroviral therapy (ART), HIV-exposed uninfected (HEU) infants have greater infectious morbidity than HIV-unexposed (HU) infants. We hypothesised that with the introduction of universal maternal ART, breastfed HEU and HU infants would have similar morbidity.
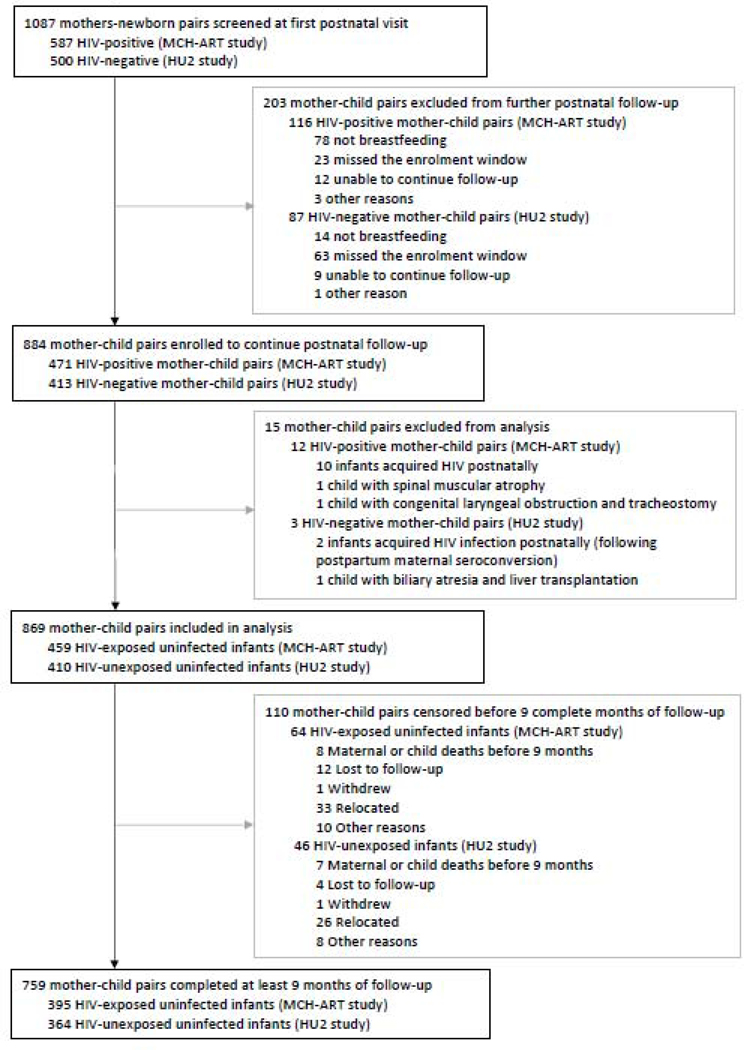
Methods: We prospectively studied a cohort of HIV-infected pregnant women initiating ART, and a parallel group of HIV-uninfected pregnant women, starting from their first antenatal care visit at the Gugulethu Midwife Obstetrics Unit in Cape Town, South Africa. All pregnant women attending their first antenatal care visit were eligible for enrolment if aged 18 years or older and planning to deliver in Cape Town, without gestational age restrictions. HIV-infected women were participants of the Maternal Child Health ART (MCH-ART) study, and HIV-uninfected women were participants of the HIV-Unexposed Uninfected (HU2) study. All enrolled women were followed up during pregnancy and through delivery. At the early neonatal visit (scheduled for the first week after birth), mother-infant pairs who practiced any breastfeeding in the first 7 days of life were eligible for further postnatal follow-up for at least 12 months post partum. HIV infection was excluded among HEU infants at ages 6 weeks and 12 months by PCR. We evaluated the effect of HIV exposure on two primary outcomes: hospitalisation (all-cause and infection-related admission to hospital) and longitudinal prevalence of child infectious illness (diarrhoea and presumed lower respiratory tract infection [LRTI]). Hospitalisation data were abstracted from routine health records. Crude and adjusted incidence rate ratios (aIRRs; with adjustment for maternal HIV disease severity, timing of ART initiation, breastfeeding, timely vaccination, and birth outcomes [gestational size and age]) for infection-related hospitalisations were calculated from Poisson regression models (with variance corrected for clustering). Prevalence of infant infectious illness was based on maternal self-report for the preceding 2 weeks of each visit, with questions based on Demographic and Health Survey (DHS) questionnaires. Infants who acquired HIV infection during follow-up were excluded from this analysis. MCH-ART is registered on ClinicalTrials.gov, NCT01933477.
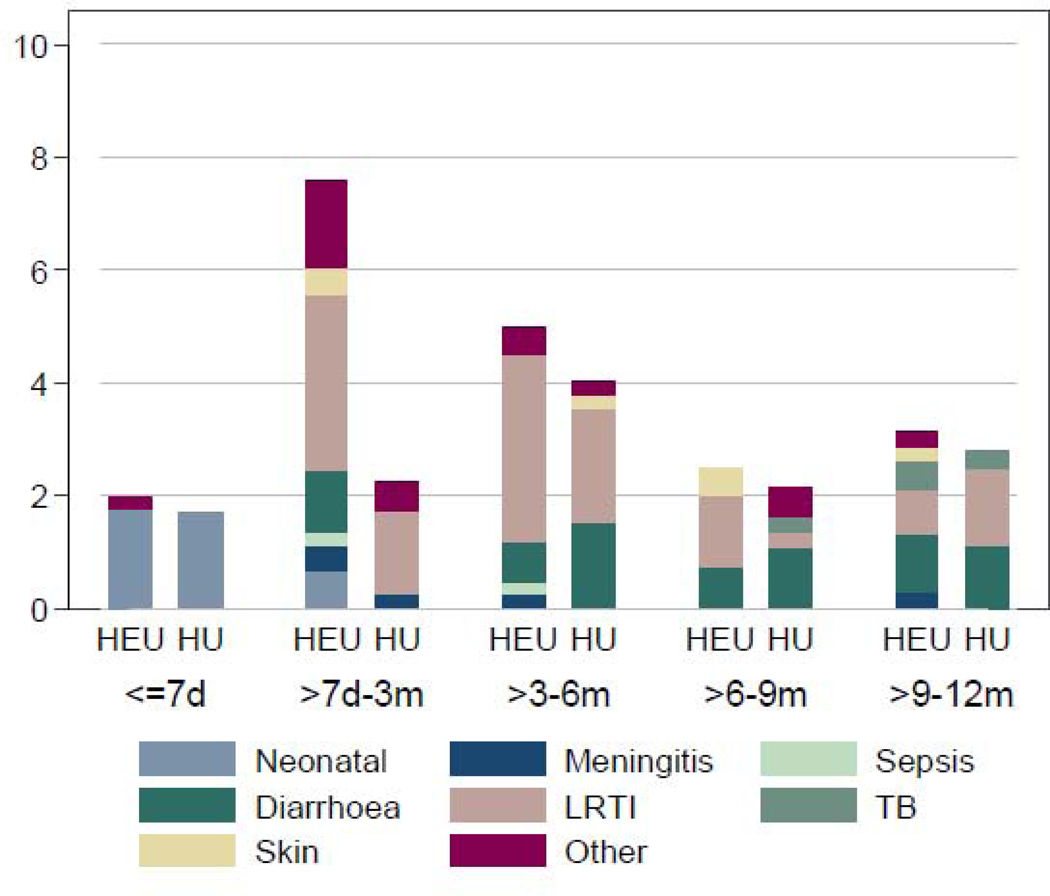
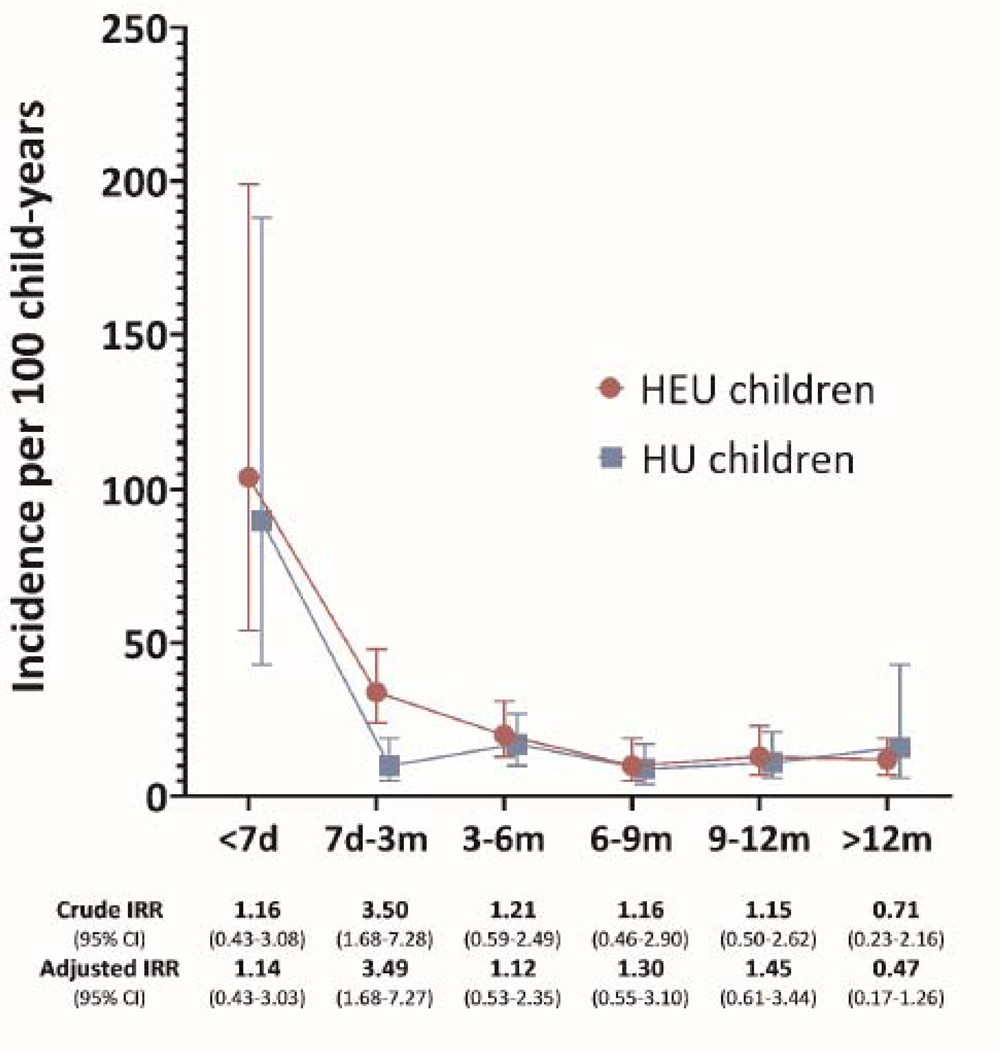
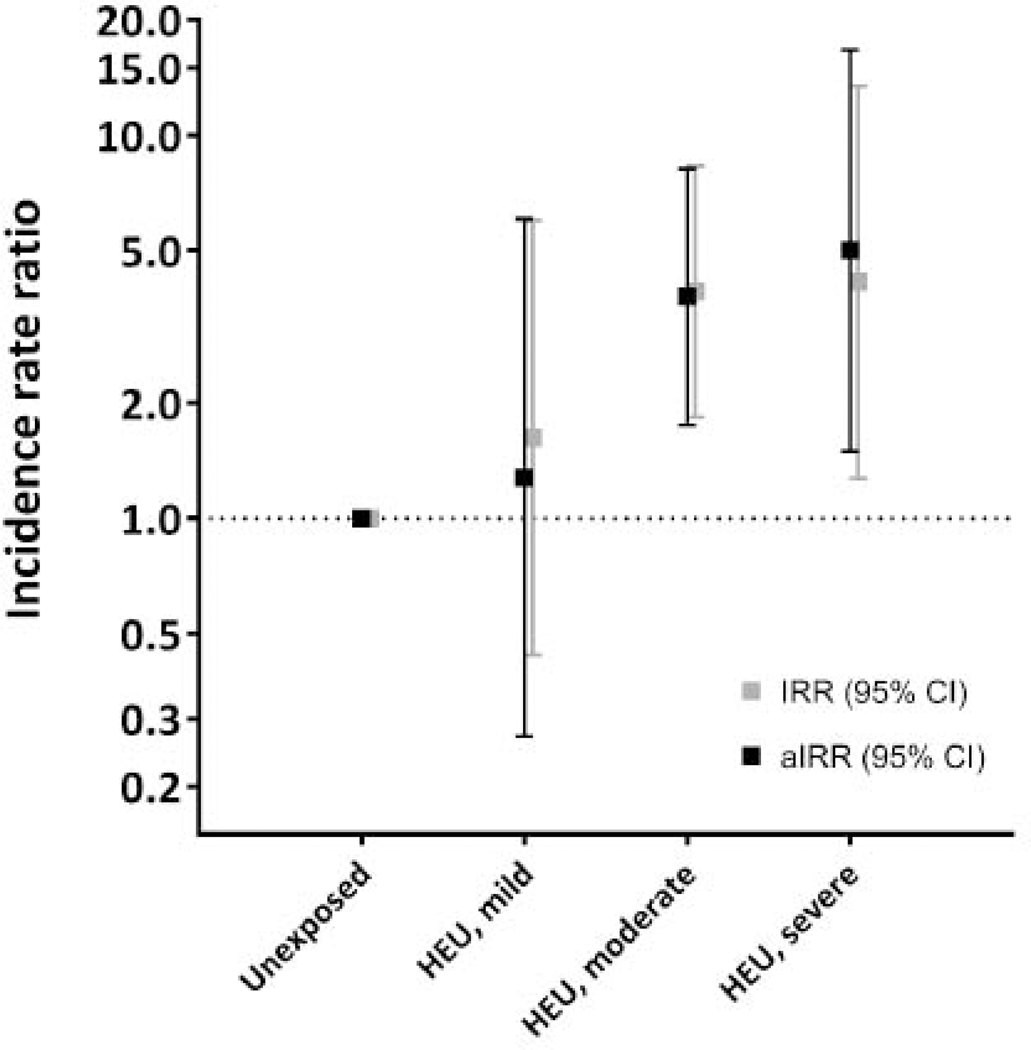
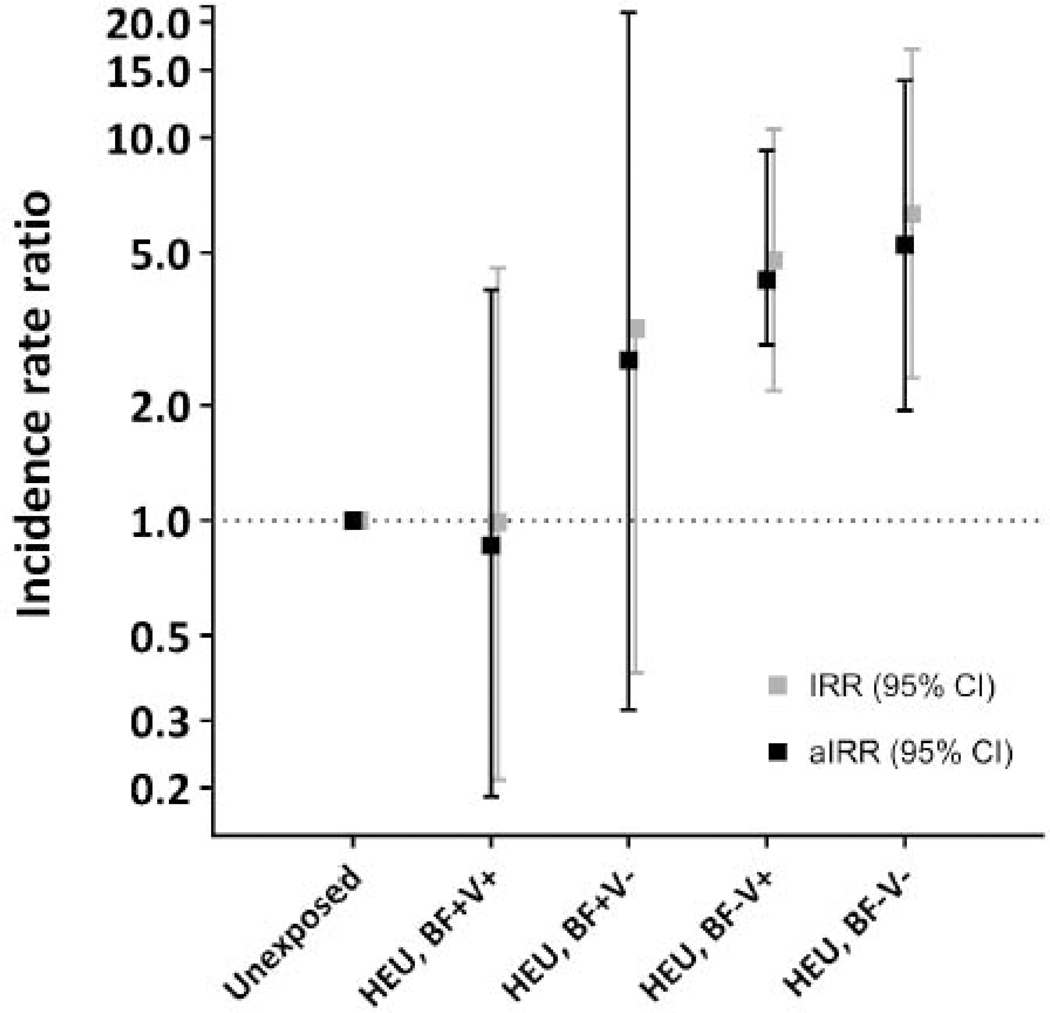
Findings: Pregnant women were recruited between March 20, 2013, and Aug 19, 2015. Mother-infant pairs (HEU, n=459; HU, n=410) were followed up for a median of 12 months until March 24, 2017. Compared with HU infants, HEU infants had more infection-related hospitalisations between the age of 8 days and 3 months (HEU, 34·2 admissions per 100 child-years [24·4-47·9] vs 9·8 per 100 child-years [95% CI 5·1-18·8]; IRR 3·50 [95% CI 1·68-7·30]), but rates were similar at other ages. In infants aged 8 days to 3 months, infection-related hospitalisations for HEU infants with healthier mothers (n=84; ART initiation at <24 weeks' gestation, CD4 count >350 cells per μL, HIV viral load <4·0 log10 copies per mL: 15·88 admissions per 100 child-years [5·12-49·23]) approximated those of HU infants (9·77 per 100 child-years [5·08-18·78]; aIRR 1·28 [0·27-6·05]). HEU infants of mothers with late ART initiation (at ≥24 weeks' gestation) and advanced disease (CD4 count ≤350 cells per μL and HIV viral load ≥4·0 log10 copies per mL; n=44) had the highest admission rate (40·44 per 100 child-years [15·18-107·74]; aIRR 5·01 [1·50-16·71]). In this age group, reduced admissions were seen in HEU infants with optimal breastfeeding (initiated within 1 h of birth and exclusive through age 3 months) and timely vaccination (required doses received within 2 weeks of indicated age; n=90; 9·63 admissions per 100 child-years [2·41-38·49]). Between birth and age 6 months, HEU infants had an almost five times greater prevalence of LRTIs than HU infants (aPR 4·69 [2·40-9·17]), and a three-times greater prevalence of diarrhoeal illness (aPR 2·93 [1·70-5·07]). After age 6 months, these associations were ameliorated.
Interpretation: Despite ART in pregnancy, breastfed HEU infants versus breastfed HU infants had transiently increased infectious morbidity risks in early infancy. However, differences were driven by factors potentially amenable to intervention, including delayed diagnosis and ART initiation in HIV-positive mothers, and suboptimal breastfeeding and vaccination of their infants.
Funding: US National Institute of Child Health and Human Development, Elizabeth Glaser Pediatric AIDS Foundation, South African Medical Research Council, Fogarty Foundation and the Office of AIDS Research.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Optimal breastfeeding for children born to mothers living with HIV.Lancet Child Adolesc Health. 2020 Mar;4(3):172-174. doi: 10.1016/S2352-4642(19)30399-2. Epub 2020 Jan 10. Lancet Child Adolesc Health. 2020. PMID: 31932245 No abstract available.
References
-
- Start Free Stay Free AIDS Free. UNAIDS report 2019. https://www.unaids.org/sites/default/files/media_asset/20190722_UNAIDS_S... (accessed 7 August 2019).
-
- le Roux SM, Abrams EJ, Nguyen K, Myer L. Clinical outcomes of HIV-exposed, HIV-uninfected children in sub-Saharan Africa. Trop Med Int Health 2016; 21(7): 829–45. - PubMed
-
- Evans C, Jones CE, Prendergast AJ. HIV-exposed, uninfected infants: new global challenges in the era of paediatric HIV elimination. Lancet Infectious Diseases, 2016. https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(16)00055... (accessed 31 August 2019). - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
