

An integrated perfusion machine preserves injured human livers for 1 week
- PMID: 31932726
- PMCID: PMC7008032
- DOI: 10.1038/s41587-019-0374-x
An integrated perfusion machine preserves injured human livers for 1 week
Abstract
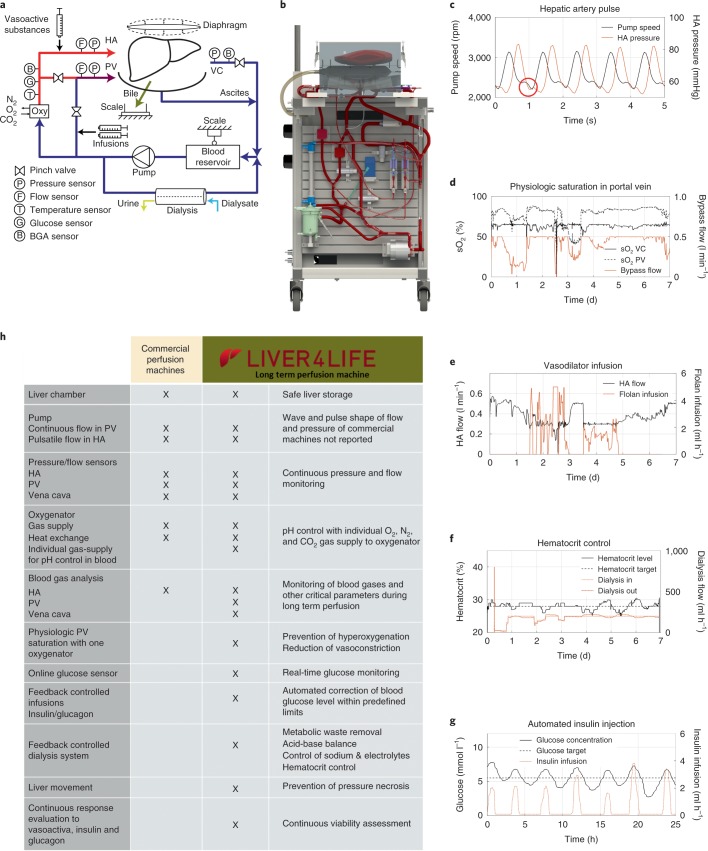
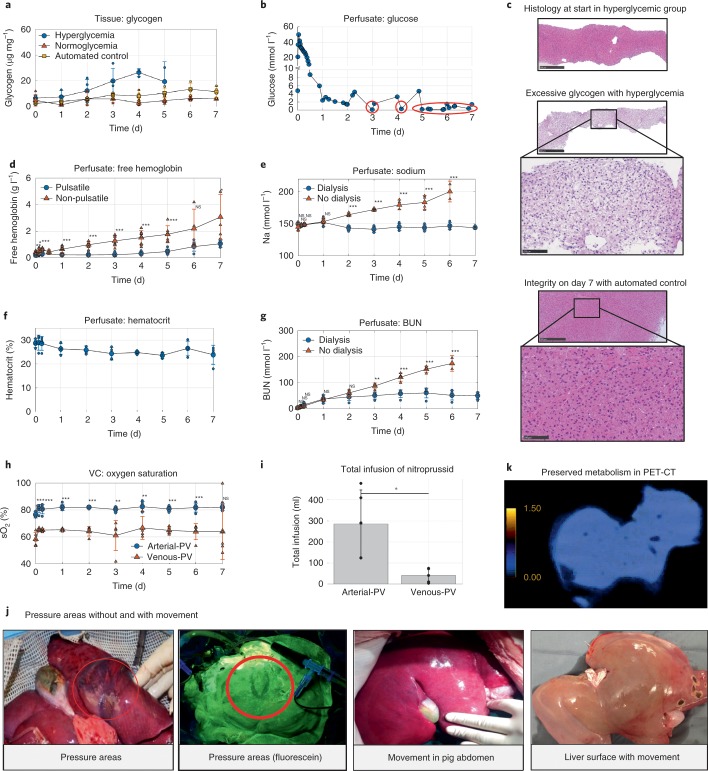
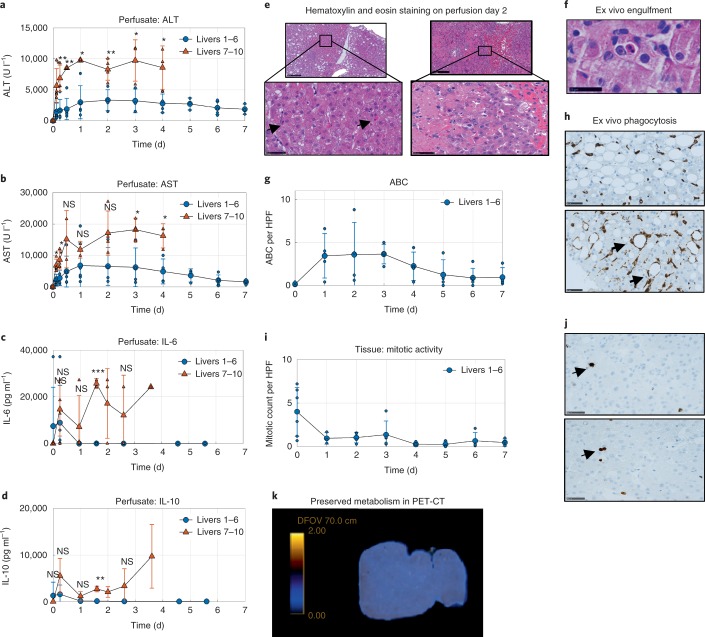
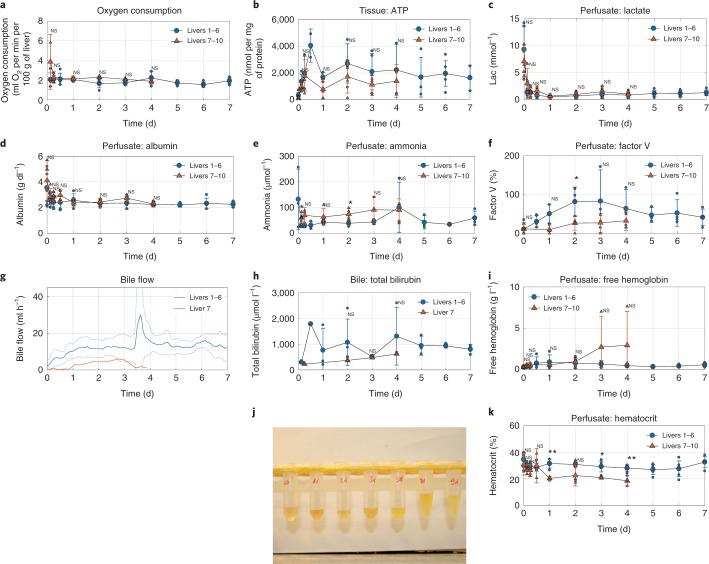
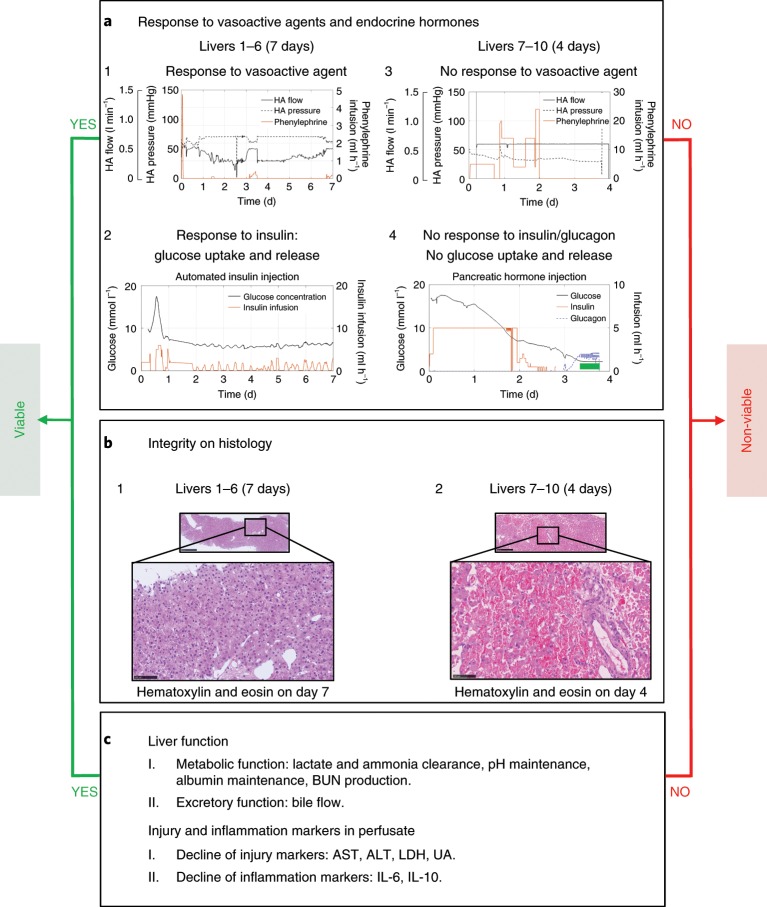
The ability to preserve metabolically active livers ex vivo for 1 week or more could allow repair of poor-quality livers that would otherwise be declined for transplantation. Current approaches for normothermic perfusion can preserve human livers for only 24 h. Here we report a liver perfusion machine that integrates multiple core physiological functions, including automated management of glucose levels and oxygenation, waste-product removal and hematocrit control. We developed the machine in a stepwise fashion using pig livers. Study of multiple ex vivo parameters and early phase reperfusion in vivo demonstrated the viability of pig livers perfused for 1 week without the need for additional blood products or perfusate exchange. We tested the approach on ten injured human livers that had been declined for transplantation by all European centers. After a 7-d perfusion, six of the human livers showed preserved function as indicated by bile production, synthesis of coagulation factors, maintained cellular energy (ATP) and intact liver structure.
Conflict of interest statement
ETH (Swiss Federal Institute of Technology in Zurich) and the University of Zurich (D.E., D.B., L.B.B., M.H., M.J.S., X.M., P.D., R. G., P.R.v.R. and P.-A.C.) have applied for a patent on this new perfusion technology (PCT/EP2019/051252).
Figures
Comment in
-
Lactate measurements in an integrated perfusion machine for human livers.Nat Biotechnol. 2020 Nov;38(11):1259. doi: 10.1038/s41587-020-0626-9. Epub 2020 Oct 26. Nat Biotechnol. 2020. PMID: 33106682 No abstract available.
-
Viability criteria assessment during liver machine perfusion.Nat Biotechnol. 2020 Nov;38(11):1260-1262. doi: 10.1038/s41587-020-0720-z. Epub 2020 Oct 26. Nat Biotechnol. 2020. PMID: 33106683 No abstract available.
-
Reply to: Lactate measurements in an integrated perfusion machine for human livers.Nat Biotechnol. 2020 Nov;38(11):1263-1264. doi: 10.1038/s41587-020-0627-8. Epub 2020 Oct 26. Nat Biotechnol. 2020. PMID: 33106684 No abstract available.
-
Long-Term Perfusion of the Liver Outside the Body: Warming Up for Ex Vivo Therapies?Hepatology. 2020 Oct;72(4):1485-1487. doi: 10.1002/hep.31474. Hepatology. 2020. PMID: 33464565 Free PMC article. No abstract available.
References
-
- Buying time for transplants. Nat. Biotechnol.35, 801 (2017). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
