

Antitumor activity of crizotinib in lung cancers harboring a MET exon 14 alteration
- PMID: 31932802
- PMCID: PMC8500676
- DOI: 10.1038/s41591-019-0716-8
Antitumor activity of crizotinib in lung cancers harboring a MET exon 14 alteration
Abstract
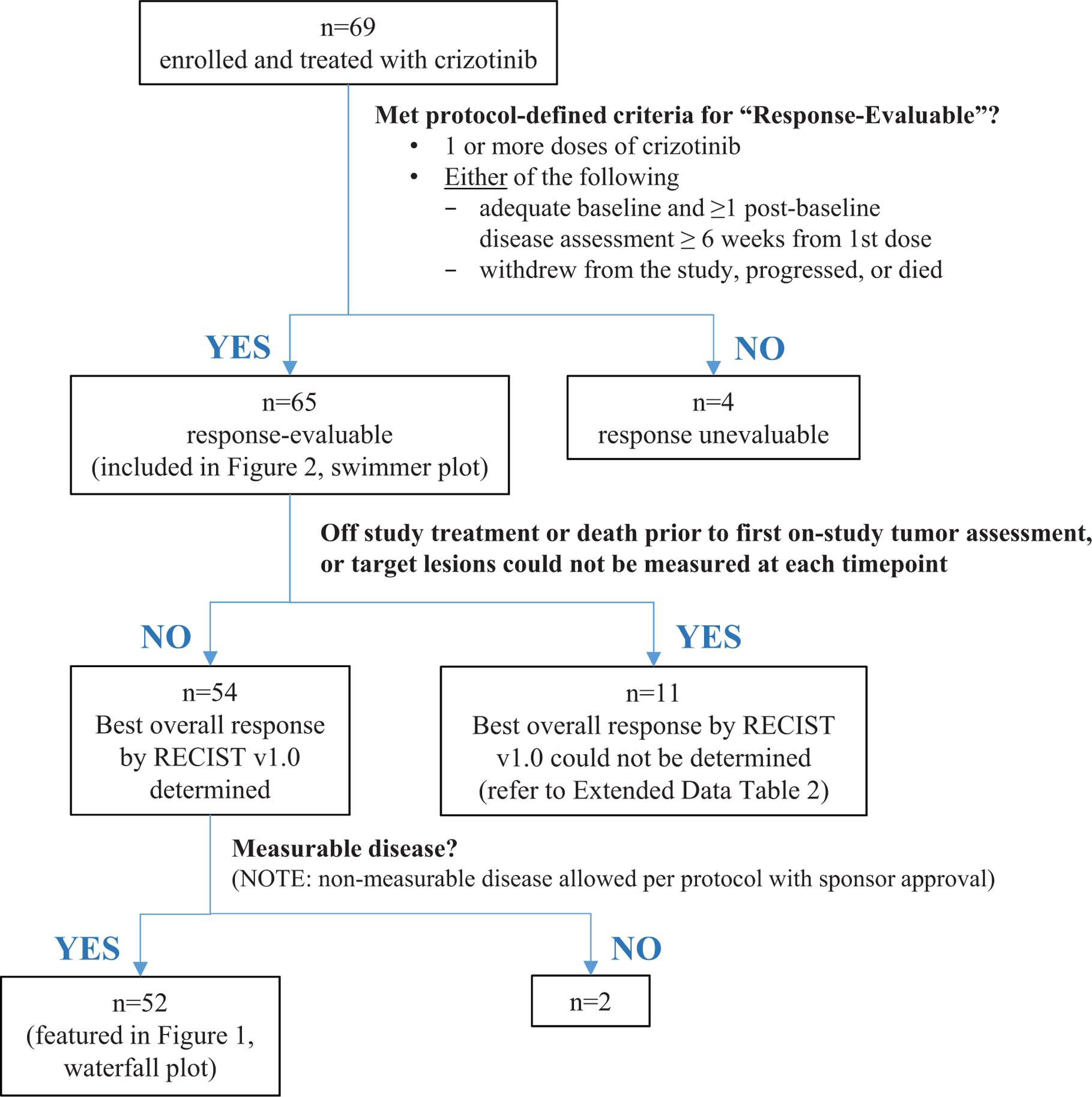
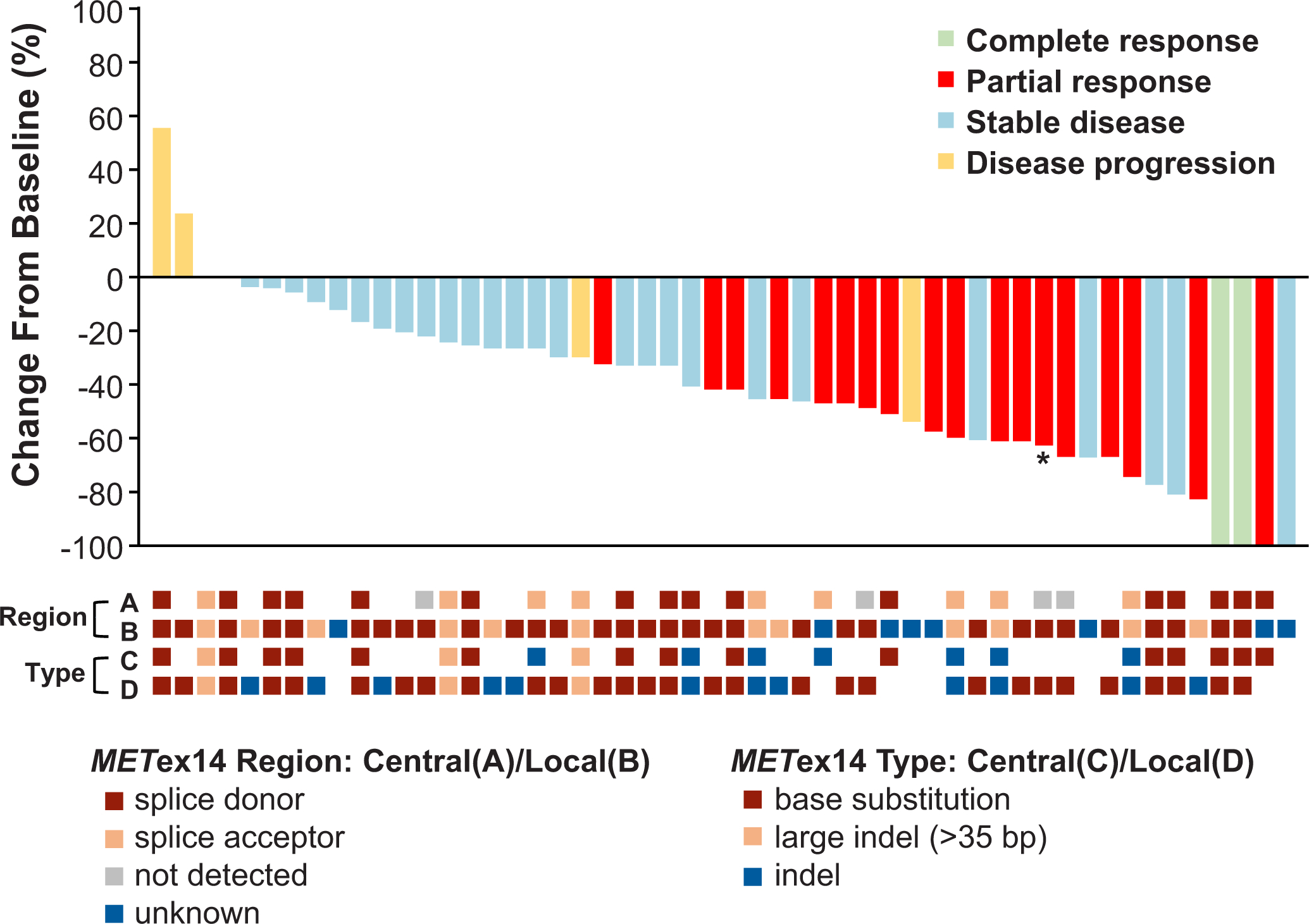
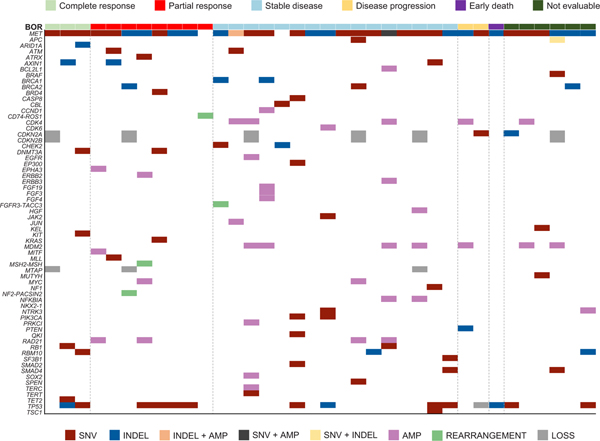
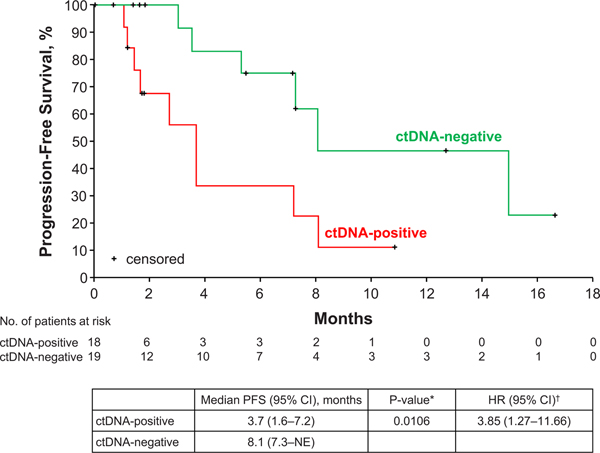
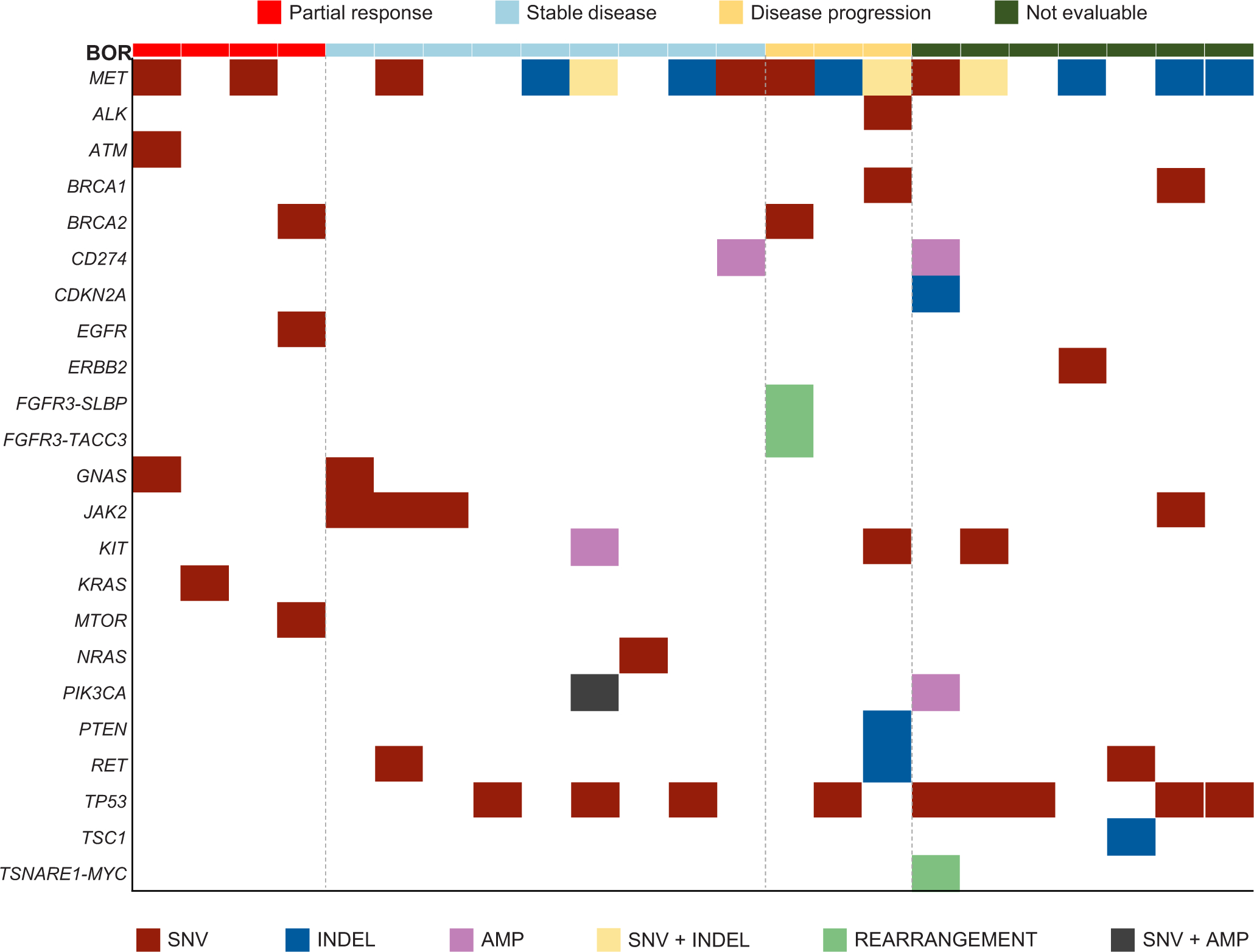
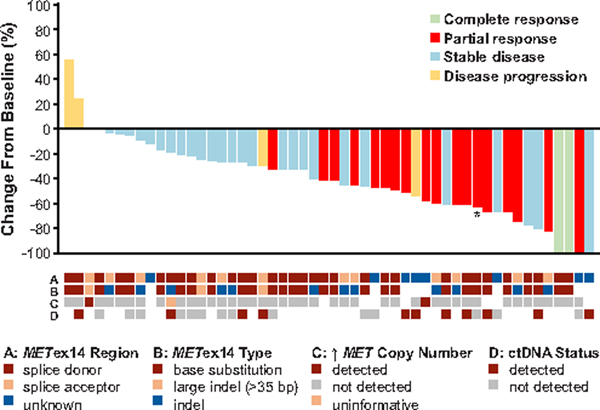
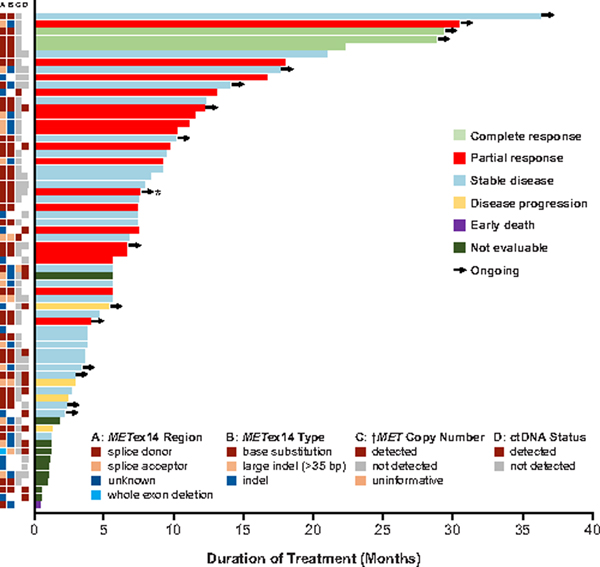
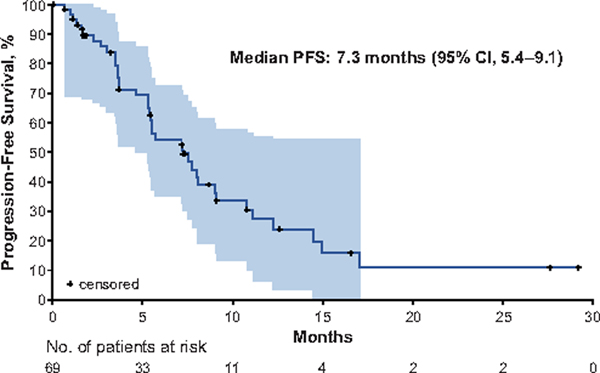
MET exon 14 alterations are oncogenic drivers of non-small-cell lung cancers (NSCLCs)1. These alterations are associated with increased MET activity and preclinical sensitivity to MET inhibition2. Crizotinib is a multikinase inhibitor with potent activity against MET3. The antitumor activity and safety of crizotinib were assessed in 69 patients with advanced NSCLCs harboring MET exon 14 alterations. Objective response rate was 32% (95% confidence interval (CI), 21-45) among 65 response-evaluable patients. Objective responses were observed independent of the molecular heterogeneity that characterizes these cancers and did not vary by splice-site region and mutation type of the MET exon 14 alteration, concurrent increased MET copy number or the detection of a MET exon 14 alteration in circulating tumor DNA. The median duration of response was 9.1 months (95% CI, 6.4-12.7). The median progression-free survival was 7.3 months (95% CI, 5.4-9.1). MET exon 14 alteration defines a molecular subgroup of NSCLCs for which MET inhibition with crizotinib is active. These results address an unmet need for targeted therapy in people with lung cancers with MET exon 14 alterations and adds to an expanding list of genomically driven therapies for oncogenic subsets of NSCLC.
Figures
Comment in
-
Multikinase Inhibitor Crizotinib Is Active in MET Exon 14-Altered Lung Cancer.Cancer Discov. 2020 Mar;10(3):337. doi: 10.1158/2159-8290.CD-RW2020-015. Epub 2020 Jan 24. Cancer Discov. 2020. PMID: 31980568
References
-
- Kong-Beltran M et al. Somatic mutations lead to an oncogenic deletion of met in lung cancer. Cancer Res. 66, 283–289 (2006). - PubMed
-
- Ma PC et al. Functional expression and mutations of c-Met and its therapeutic inhibition with SU11274 and small interfering RNA in non-small cell lung cancer. Cancer Res. 65, 1479–1488 (2005). - PubMed
-
- Cui JJ et al. Structure based drug design of crizotinib (PF-02341066), a potent and selective dual inhibitor of mesenchymal-epithelial transition factor (c-MET) kinase and anaplastic lymphoma kinase (ALK). J. Med. Chem. 54, 6342–6363 (2011). - PubMed
-
- Awad MM et al. MET Exon 14 Mutations in Non-Small-Cell Lung Cancer Are Associated With Advanced Age and Stage-Dependent MET Genomic Amplification and c-Met Overexpression. J. Clin. Oncol. 34, 721–730 (2016). - PubMed
-
- Tong JH et al. MET amplification and exon 14 splice site mutation define unique molecular subgroups of Non-small Cell Lung Carcinoma with poor prognosis. Clin. Cancer Res. 22, 3048–3056 (2016). - PubMed
Methods References
-
- Frampton GM et al. Activation of MET via diverse exon 14 splicing alterations occurs in multiple tumor types and confers clinical sensitivity to MET inhibitors. Cancer Discov. 5, 850–859 (2015). - PubMed
-
- Palma NA et al. Frequency of MET amplification determined by comprehensive next-generation sequencing (NGS) in multiple solid tumors and implications for use of MET inhibitors. J. Clin. Oncol. 31, doi: 10.1200/jco.2013.31.15_suppl.11068 (2013). - DOI
-
- Oken MM et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 5, 649–655 (1982). - PubMed
-
- Therasse P et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J. Natl. Cancer Inst. 92, 205–216 (2000). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
