

Complement blockade for TA-TMA: lessons learned from a large pediatric cohort treated with eculizumab
- PMID: 31932840
- PMCID: PMC7099329
- DOI: 10.1182/blood.2019004218
Complement blockade for TA-TMA: lessons learned from a large pediatric cohort treated with eculizumab
Abstract
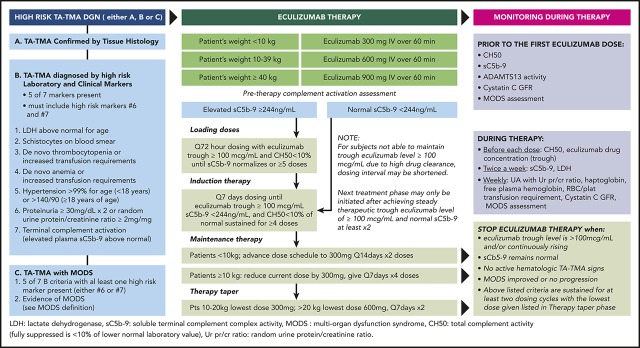
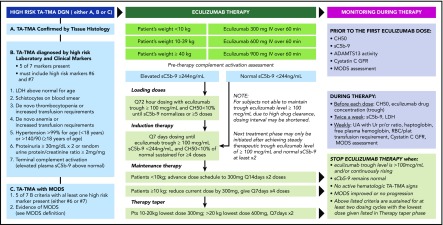
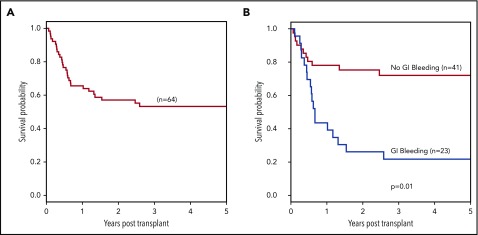
Overactivated complement is a high-risk feature in hematopoietic stem cell transplant (HSCT) recipients with transplant-associated thrombotic microangiopathy (TA-TMA), and untreated patients have dismal outcomes. We present our experience with 64 pediatric HSCT recipients who had high-risk TA-TMA (hrTA-TMA) and multiorgan injury treated with the complement blocker eculizumab. We demonstrate significant improvement to 66% in 1-year post-HSCT survival in treated patients from our previously reported untreated cohort with same hrTA-TMA features that had 1-year post-HSCT survival of 16.7%. Responding patients benefited from a brief but intensive course of eculizumab using pharmacokinetic/pharmacodynamic-guided dosing, requiring a median of 11 doses of eculizumab (interquartile range [IQR] 7-20). Treatment was discontinued because TA-TMA resolved at a median of 66 days (IQR 41-110). Subjects with higher complement activation measured by elevated blood sC5b-9 at the start of treatment were less likely to respond (odds ratio, 0.15; P = .0014) and required more doses of eculizumab (r = 0.43; P = .0004). Patients with intestinal bleeding had the fastest eculizumab clearance, required the highest number of eculizumab doses (20 vs 9; P = .0015), and had lower 1-year survival (44% vs 78%; P = .01). Over 70% of survivors had proteinuria on long-term follow-up. The best glomerular filtration rate (GFR) recovery in survivors was a median 20% lower (IQR, 7.3%-40.3%) than their pre-HSCT GFR. In summary, complement blockade with eculizumab is an effective therapeutic strategy for hrTA-TMA, but some patients with severe disease lacked a complete response, prompting us to propose early intervention and search for additional targetable endothelial injury pathways.
© 2020 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: S.J., S.M.D., B.L.L., and K.M. have a US Provisional Patent Application pending. The remaining authors declare no competing financial interests.
Figures
Comment in
-
Compliments to complement blockade for TA-TMA.Blood. 2020 Mar 26;135(13):981-983. doi: 10.1182/blood.2020005040. Blood. 2020. PMID: 32219351 No abstract available.
References
-
- Moiseev IS, Tsvetkova T, Aljurf M, et al. Clinical and morphological practices in the diagnosis of transplant-associated microangiopathy: a study on behalf of Transplant Complications Working Party of the EBMT. Bone Marrow Transplant. 2019;54(7):1022-1028. - PubMed
-
- Gavriilaki E, Sakellari I, Batsis I, et al. Transplant-associated thrombotic microangiopathy: Incidence, prognostic factors, morbidity, and mortality in allogeneic hematopoietic cell transplantation. Clin Transplant. 2018;32(9):e13371. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
