

Comparison of three different diffractıve multifocal intraocular lenses with a +2.5, +3.0, and +3.75 diopter additıon power
- PMID: 31933530
- PMCID: PMC6950979
- DOI: 10.1016/j.sjopt.2019.09.007
Comparison of three different diffractıve multifocal intraocular lenses with a +2.5, +3.0, and +3.75 diopter additıon power
Abstract
Purpose: To compare the functional outcomes and astigmatic tolerability after implantation of multifocal intraocular lenses (IOLs) with a +2.5, +3.0, and +3.75 diopter (D) addition power.
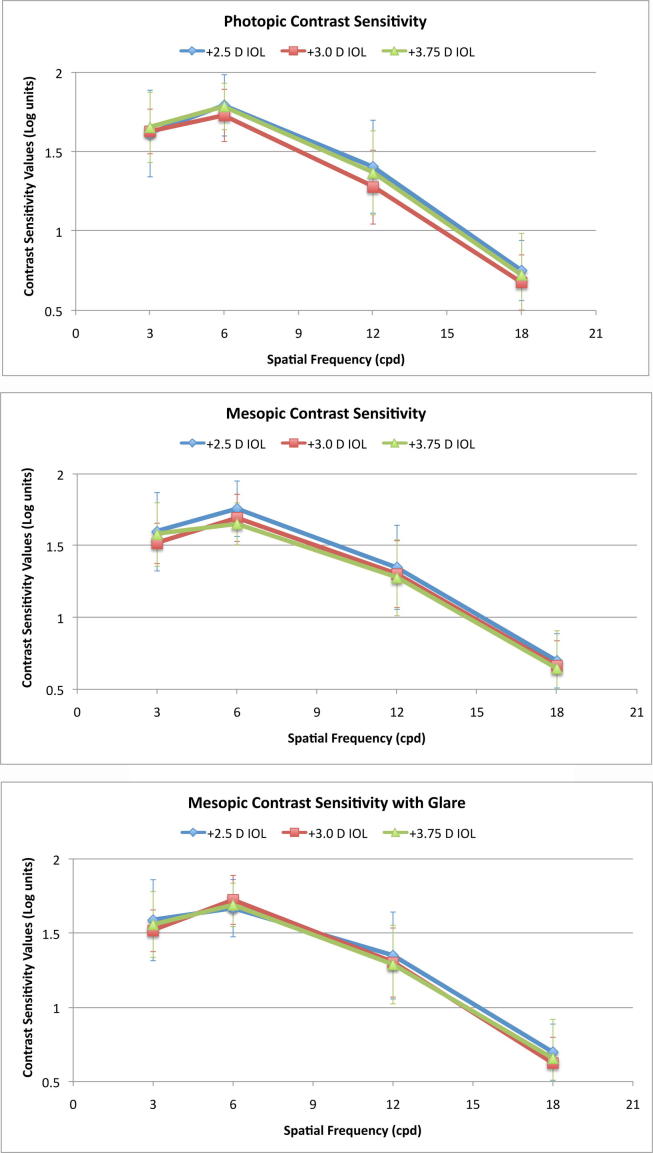
Methods: This study included 122 eyes of 61 patients who had bilateral cataract extraction and implantation of diffractive aspheric multifocal acrylic IOLs with +2.5 D (+2.5 group), +3.0 D (+3.0 group), and +3.75 D (+3.75 group) addition powers. 1-year after surgery, distance corrected near (DNVA) and intermediate (DIVA) visual acuities at 32, 40, 45, 50, 55, and 60 cm; and contrast sensitivity measurements under photopic, mesopic and mesopic with glare conditions; spherical and astigmatic defocus testing; distance-intermediate-near vision patient satisfaction levels; spectacle dependance; patient-reported outcomes were assessed binocularly.
Results: The +2.50 D group had better DIVA than both +3.0 group and +3.75 groups at 45 cm, 50 cm, 55 cm, and 60 cm (p < 0.05). The +3.75 group had better DNVA than both +2.5 and +3.0 IOL groups at 32 cm (p < 0.05). There was no significant difference in mean contrast values at all frequencies between three IOL groups (p > 0.05). The +2.50 D group showed better astigmatic tolerability than +3.00 group (at 2.00 D) and +3.75 group (at 1.50 D, and at 2.00 D) (p < 0.05).
Conclusion: Multifocal IOLs with +2.5 add power have better intermediate vision, but worse near vision compared to multifocal IOLs with +3.00 D and +3.75 D add power. Multifocal IOLs with +2.50 D add power tend to have better astigmatic defocus tolerability than multifocal IOLs with +3.00 D and +3.75 D add powers.
Keywords: Astigmatism; Cataract; Intraocular lens; Phacoemulsification; Presbyopia.
© 2019 The Authors.
Conflict of interest statement
The authors have no financial interest in any of the issues contained in this article and have no proprietary interest in the development of marketing of or materials used in this study. The manuscript was presented as a free paper at the 33rd Congress of the European Society of Cataract and Refractive Surgeons (ESCRS) on the 8th of September, 2015 in Barcelona, Spain.
Figures






References
-
- Braga-Mele R., Chang D., Dewey S. Multifocal intraocular lenses: relative indications and contraindications for implantation. J Cataract Refract Surg. 2014;40(2):313–322. - PubMed
-
- Olson R.J., Werner L., Mamalis N., Cionni R. New intraocular lens technology. Am J Ophthalmol. 2005;140(4):709–716. - PubMed
-
- Cillino G., Casuccio A., Pasti M., Bono V., Mencucci R., Cillino S. Working-age cataract patients: visual results, reading performance, and quality of life with three diffractive multifocal intraocular lenses. Ophthalmology. 2014;121(1):34–44. - PubMed
-
- Artigas J.M., Menezo J.L., Peris C., Felipe A., Díaz-Llopis M. Image quality with multifocal intraocular lenses and the effect of pupil size: comparison of refractive and hybrid refractive-diffractive designs. J Cataract Refract Surg. 2007;33(12):2111–2117. - PubMed
LinkOut - more resources
Full Text Sources
