

Visual Outcomes of Plasma Exchange Treatment of Steroid-Refractory Optic Neuritis: A Retrospective Monocentric Analysis
- PMID: 31933571
- PMCID: PMC6944937
- DOI: 10.1159/000504027
Visual Outcomes of Plasma Exchange Treatment of Steroid-Refractory Optic Neuritis: A Retrospective Monocentric Analysis
Abstract
Introduction: In acute inflammatory optic neuritis (ON) as a typical onset of multiple sclerosis (MS), only few studies have investigated plasma exchange (PLEX) as a sequential treatment after insufficient response to high-dose intravenous glucocorticosteroids. Therefore, we aimed to investigate treatment outcome on visual acuity (VA) with PLEX in patients with steroid-refractory ON.
Methods: In our retrospective monocentric study, medical records were screened for patients with acute ON as their first relapse with sequential MS diagnosis or with an established MS diagnosis from the Bern University Hospital (Switzerland) that were treated with PLEX between 2016 and 2018 due to lacking steroid response. VA prior to steroid administration, and before and after PLEX were assessed and compared using the Friedman multiple comparison test.
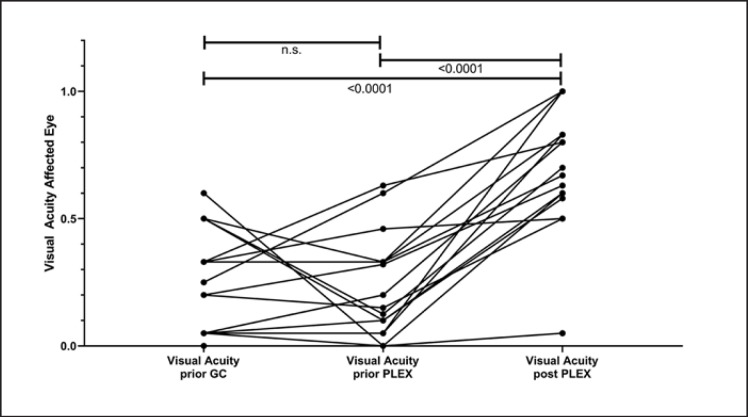
Results: In total, 18 patients were included in the analysis. Interval from symptom onset to PLEX was 20.3 days (mean, 95% CI 14.8-25.9). Relevant functional improvement (VA of ≥0.5, after a mean of 15.9 (13.3-18.5) days after start of PLEX) was detected in 16/18 (88.9%) with a significant amelioration as compared to VA before glucocorticosteroids and before PLEX (p < 0.0001). VA improvement at a later time point (38.1 weeks, 25.2-51.0) was present in 15/16 (93.8%) patients. No serious adverse events were detected. PLEX could be performed via peripheral access in 13/18 patients (72.2%).
Conclusion: Our study demonstrates significant improvements of VA with PLEX in a cohort of MS patients with steroid-refractory ON. High response rates may be due to the timely treatment initiation. Despite the small sample size, our data support the early use of PLEX in steroid-refractory ON with a favorable safety profile.
Keywords: Apheresis; Multiple sclerosis; Relapse; Visual acuity.
Copyright © 2019 by S. Karger AG, Basel.
Conflict of interest statement
A. Miclea, N. Skorupka, C. Bocksrucker, B. Mansouri Taleghani report no disclosures. K.A. Jalowiec received travel grants from Amgen, Pfizer, Novartis, not related to this work. N. Kamber received travel grants from Biogen, Merck, Genzyme, and Roche and speaker honoraria from Biogen and Roche, not related to this work. A. Chan has received personal compensation for activities with Bayer, Biogen, Genzyme, Merck, Novartis, Roche, Teva. He received research support from the Swiss National Fonds (SNF, No. 310030_172952), Genzyme, and UCB. He serves in the editorial board for Clinical and Translational Neuroscience and the Journal of International Medical Research. R. Hoepner received research and travel grants from Novartis and Biogen Idec. He also received speaker honoraria from Biogen, Novartis, Merck, and Almirall. He is supported by the Swiss Multiple Sclerosis Society. A. Salmen received speaker honoraria and/or travel compensation for activities with Almirall Hermal GmbH, Biogen, Merck, Novartis, Roche, and Sanofi Genzyme, none related to this work.
Figures
References
-
- Toosy AT, Mason DF, Miller DH. Optic neuritis. Lancet Neurol. 2014 Jan;13((1)):83–99. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
