

Proliferative myositis and nodular fasciitis: a retrospective study with clinicopathologic and radiologic correlation
- PMID: 31933833
- PMCID: PMC6949867
Proliferative myositis and nodular fasciitis: a retrospective study with clinicopathologic and radiologic correlation
Abstract
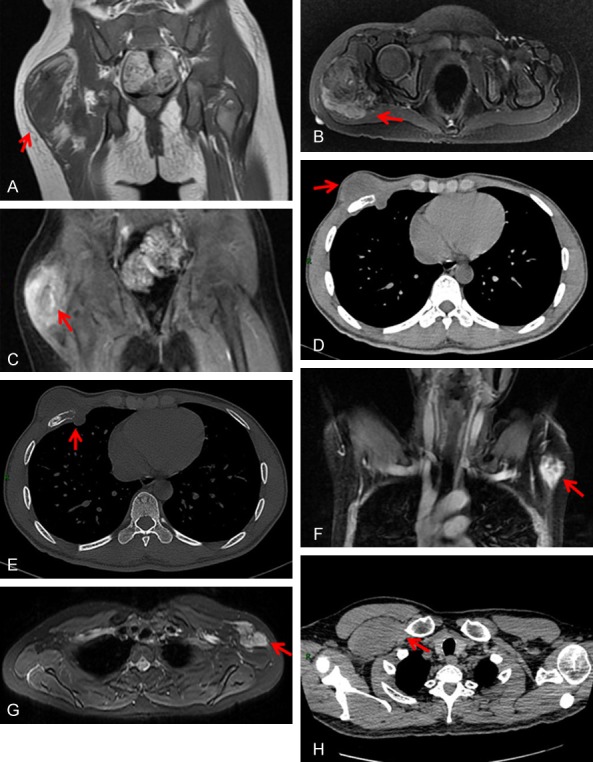
Proliferative myositis (PM) and nodular fasciitis (NF) are two diseases easily misdiagnosed as cancer, often promoting unnecessary invasive procedures. To make accurate diagnoses of PM and NF and for the differential diagnosis between them, we performed a retrospective study to evaluate the roles of the clinical, radiologic, and pathologic characteristics of PM and NF. With an emphasis on the clinicopathologic and radiologic characteristics, we conducted a retrospective study of 8 cases of PM and 64 cases of NF that were diagnosed between 2012 and 2018. According to MRI findings, the lesions of PM and NF appeared as homogeneous masses with homogenous hypointensity or isointensity on T1-weighted images and as moderately or markedly hyperintense signals on T2-weighted images compared to skeletal muscle. In terms of histopathologic features, the differences between PM and NF mainly consisted of the presence of ganglion-like myofibroblasts with vesicular nuclei and basophilic cytoplasm in PM. The areas abundant in myxoid stroma with inflammatory infiltration that did not have abundant ganglion-like cells suggest NF. Immunohistochemically, the spindle-shaped cells of PM stained positive for smooth muscle actin (SMA), while the ganglion-like cells were negative. The spindle-shaped cells of NF showed diffuse expression of SMA, calponin, and vimentin. Our comprehensive study further demonstrated that PM and NF had a wide clinicopathologic and radiologic spectrum. Correlation with the clinical, radiologic and pathologic characteristics may help clinicians and pathologists make accurate diagnoses.
Keywords: Proliferative myositis; clinical characteristics; nodular fasciitis; pathology; radiological characteristics.
IJCEP Copyright © 2019.
Conflict of interest statement
None.
Figures

References
-
- Jarraya M, Parva P, Stone M, Klein MJ, Guermazi A. Atypical proliferative myositis: original MR description with pathologic correlation: case report. Skeletal Radiol. 2014;43:1155–1159. - PubMed
-
- de Schepper AM, Vandevenne JE. Tumors of connective tissue. Imaging of Soft Tissue Tumors. 2006:167–202.
-
- Hseu A, Watters K, Perez-Atayde A, Silvera VM, Rahbar R. Pediatric nodular fasciitis in the head and neck: evaluation and management. JAMA Otolaryngol Head Neck Surg. 2015;141:54–59. - PubMed
-
- Wang XL, De Schepper AM, Vanhoenacker F, De Raeve H, Gielen J, Aparisi F, Rausin L, Somville J. Nodular fasciitis: correlation of MRI findings and histopathology. Skeletal Radiol. 2002;31:155–161. - PubMed
-
- Dinauer PA, Brixey CJ, Moncur JT, Fanburgsmith JC, Murphey MD. Pathologic and MR imaging features of benign fibrous soft-tissue tumors in adults. Radiographics. 2007;27:173–187. - PubMed
LinkOut - more resources
Full Text Sources