

Five-year results of the BEGEV salvage regimen in relapsed/refractory classical Hodgkin lymphoma
- PMID: 31935284
- PMCID: PMC6960479
- DOI: 10.1182/bloodadvances.2019000984
Five-year results of the BEGEV salvage regimen in relapsed/refractory classical Hodgkin lymphoma
Abstract
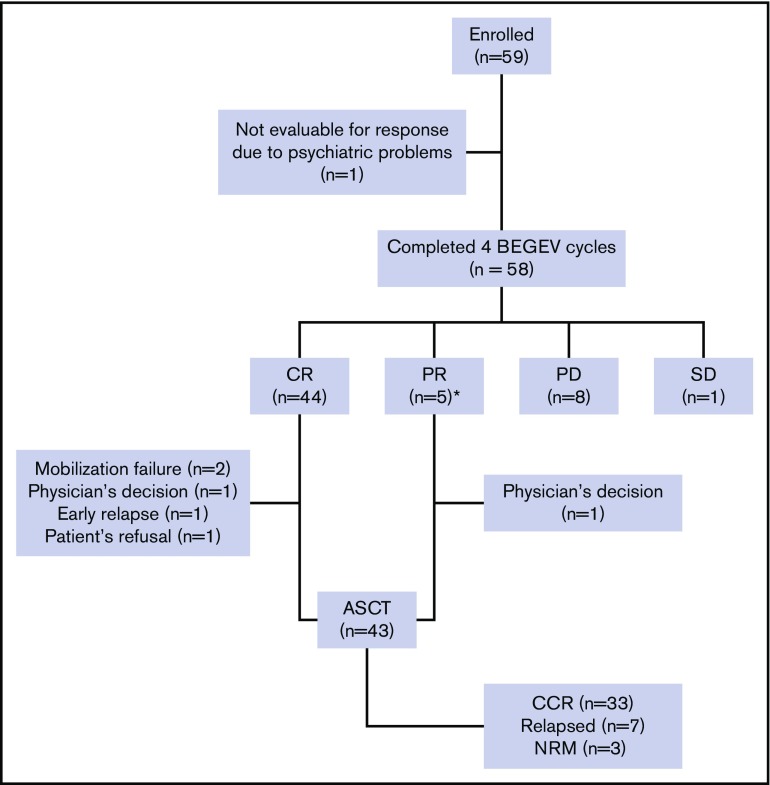
The complete remission (CR) rate achieved with induction chemotherapy prior to autologous stem cell transplantation (ASCT) represents the strongest prognostic factor in relapsed/refractory (R/R) classical Hodgkin lymphoma (cHL). By inducing a CR rate of 75%, the bendamustine, gemcitabine, vinorelbine (BEGEV) regimen represents an optimal chemotherapy regimen prior to ASCT. Presented here are the 5-year results of BEGEV followed by ASCT in R/R cHL. With a median follow-up of 5 years, progression-free survival (PFS) and overall survival (OS) for the whole series (n = 59) were 59% and 78%, respectively. ASCT was performed in 43 of 49 responding patients (73% by intention to treat [ITT]; 88% by response to BEGEV) and resulted in 33 with continuous CR (56% by ITT; 77% of transplanted patients), 7 with disease relapse, and 3 with nonrelapse mortality. For patients who received transplants, the 5-year PFS and OS were 77% and 91%, respectively, with no significant difference between relapsed and refractory patients. No patient experienced secondary leukemia or myelodysplasia. In summary, the long-term efficacy data, the benefits for both relapsed and refractory patients, and the excellent safety profile provide a strong rationale for further development of the BEGEV regimen. This trial was registered at EudraCT as #2010-022169-91 and at www.clinicaltrials.gov as #NCT01884441.
© 2020 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: A.S. reports receiving honoraria for speaker engagements and scientific advisory fees from Bristol-Myers Squibb, Servier, Gilead, Pfizer, Eisai, Bayer, Merck Sharp & Dohme, ArQule, Takeda, Roche, AbbVie, Amgen, Celgene, AstraZeneca, Pfizer, Lilly, Sandoz, and Novartis. A. Pulsoni reports receiving personal fees from Roche, Merck Sharp & Dohme, Pfizer, Sandoz, Takeda, Gilead, and Bristol-Myers Squibb. F.M. reports receiving nonfinancial support from Roche, Takeda, and Celgene and personal fees from Janssen and Gilead. S.L. reports personal fees from Roche, Celgene, Teva Pharmaceuticals, Gilead Sciences, and Takeda Pharmaceuticals. C.C.-S. reports receiving honoraria for speaker engagements from Bristol-Myers Squibb, Merck Sharp & Dohme, Amgen, Janssen Oncology, and AstraZeneca, and scientific advisory fees from Sanofi, ADC Therapeutics, Servier, Boehringer Ingelheim, Novartis, Roche, Genenta Science srl, and Rhizen Pharmaceuticals. The remaining authors declare no competing financial interests.
Figures


References
-
- Linch DC, Winfield D, Goldstone AH, et al. . Dose intensification with autologous bone-marrow transplantation in relapsed and resistant Hodgkin’s disease: results of a BNLI randomised trial. Lancet. 1993;341(8852):1051-1054. - PubMed
-
- Schmitz N, Pfistner B, Sextro M, et al. ; Lymphoma Working Party of the European Group for Blood and Marrow Transplantation . Aggressive conventional chemotherapy compared with high-dose chemotherapy with autologous haemopoietic stem-cell transplantation for relapsed chemosensitive Hodgkin’s disease: a randomised trial. Lancet. 2002;359(9323):2065-2071. - PubMed
-
- Moskowitz CH, Nimer SD, Zelenetz AD, et al. . A 2-step comprehensive high-dose chemoradiotherapy second-line program for relapsed and refractory Hodgkin disease: analysis by intent to treat and development of a prognostic model. Blood. 2001;97(3):616-623. - PubMed
-
- Josting A, Rudolph C, Reiser M, et al. ; Participating Centers . Time-intensified dexamethasone/cisplatin/cytarabine: an effective salvage therapy with low toxicity in patients with relapsed and refractory Hodgkin’s disease. Ann Oncol. 2002;13(10):1628-1635. - PubMed
