

Consensus regarding diagnosis and management of atypical hemolytic uremic syndrome
- PMID: 31935318
- PMCID: PMC6960041
- DOI: 10.3904/kjim.2019.388
Consensus regarding diagnosis and management of atypical hemolytic uremic syndrome
Abstract
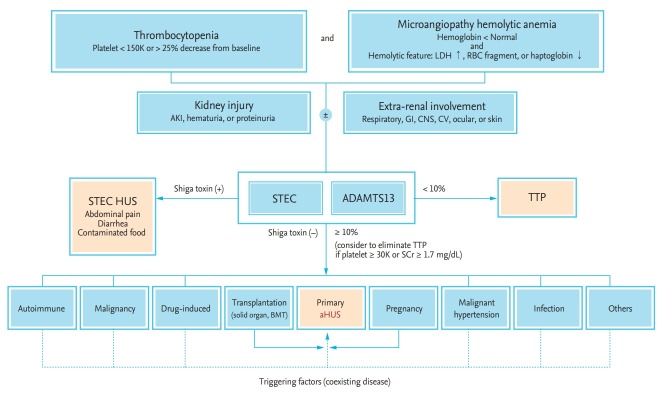
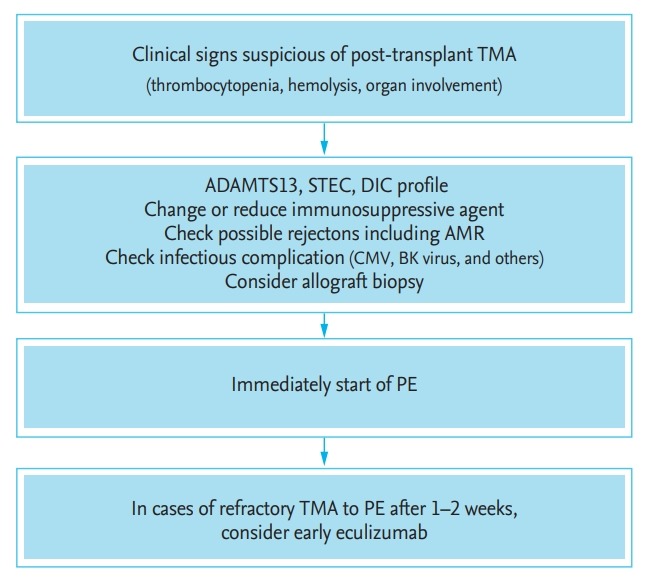
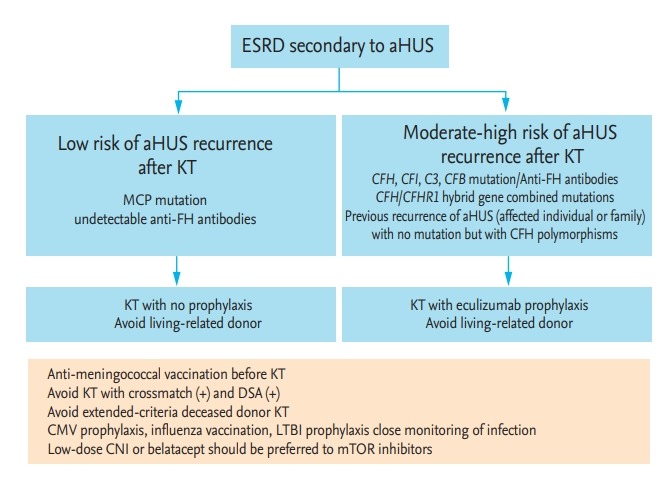
Thrombotic microangiopathy (TMA) is defined by specific clinical characteristics, including microangiopathic hemolytic anemia, thrombocytopenia, and pathologic evidence of endothelial cell damage, as well as the resulting ischemic end-organ injuries. A variety of clinical scenarios have features of TMA, including infection, pregnancy, malignancy, autoimmune disease, and medications. These overlapping manifestations hamper differential diagnosis of the underlying pathogenesis, despite recent advances in understanding the mechanisms of several types of TMA syndrome. Atypical hemolytic uremic syndrome (aHUS) is caused by a genetic or acquired defect in regulation of the alternative complement pathway. It is important to consider the possibility of aHUS in all patients who exhibit TMA with triggering conditions because of the incomplete genetic penetrance of aHUS. Therapeutic strategies for aHUS are based on functional restoration of the complement system. Eculizumab, a monoclonal antibody against the terminal complement component 5 inhibitor, yields good outcomes that include prevention of organ damage and premature death. However, there remain unresolved challenges in terms of treatment duration, cost, and infectious complications. A consensus regarding diagnosis and management of TMA syndrome would enhance understanding of the disease and enable treatment decision-making.
Keywords: Atypical hemolytic uremic syndrome; Complement pathway, alternative; Diagnosis, differential; Eculizumab; Thrombotic microangiopathies.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Moake JL. Thrombotic microangiopathies. N Engl J Med. 2002;347:589–600. - PubMed
-
- Gasser C, Gautier E, Steck A, Siebenmann RE, Oechslin R. Hemolytic-uremic syndrome: bilateral necrosis of the renal cortex in acute acquired hemolytic anemia. Schweiz Med Wochenschr. 1955;85:905–909. - PubMed
-
- Moake JL, Rudy CK, Troll JH, et al. Unusually large plasma factor VIII:von Willebrand factor multimers in chronic relapsing thrombotic thrombocytopenic purpura. N Engl J Med. 1982;307:1432–1435. - PubMed
-
- Karmali MA, Petric M, Lim C, Fleming PC, Arbus GS, Lior H. The association between idiopathic hemolytic uremic syndrome and infection by verotoxin-producing Escherichia coli. J Infect Dis. 1985;151:775–782. - PubMed
-
- Mele C, Remuzzi G, Noris M. Hemolytic uremic syndrome. Semin Immunopathol. 2014;36:399–420. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources