

Incidence and Predictors of Major Adverse Cardiovascular Events in Patients With Established Atherosclerotic Disease or Multiple Risk Factors
- PMID: 31937196
- PMCID: PMC7033849
- DOI: 10.1161/JAHA.119.014402
Incidence and Predictors of Major Adverse Cardiovascular Events in Patients With Established Atherosclerotic Disease or Multiple Risk Factors
Abstract
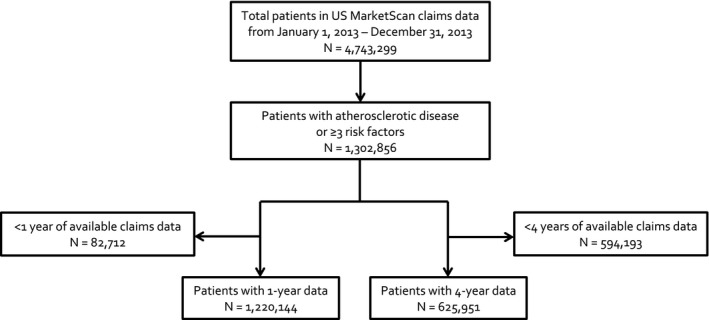
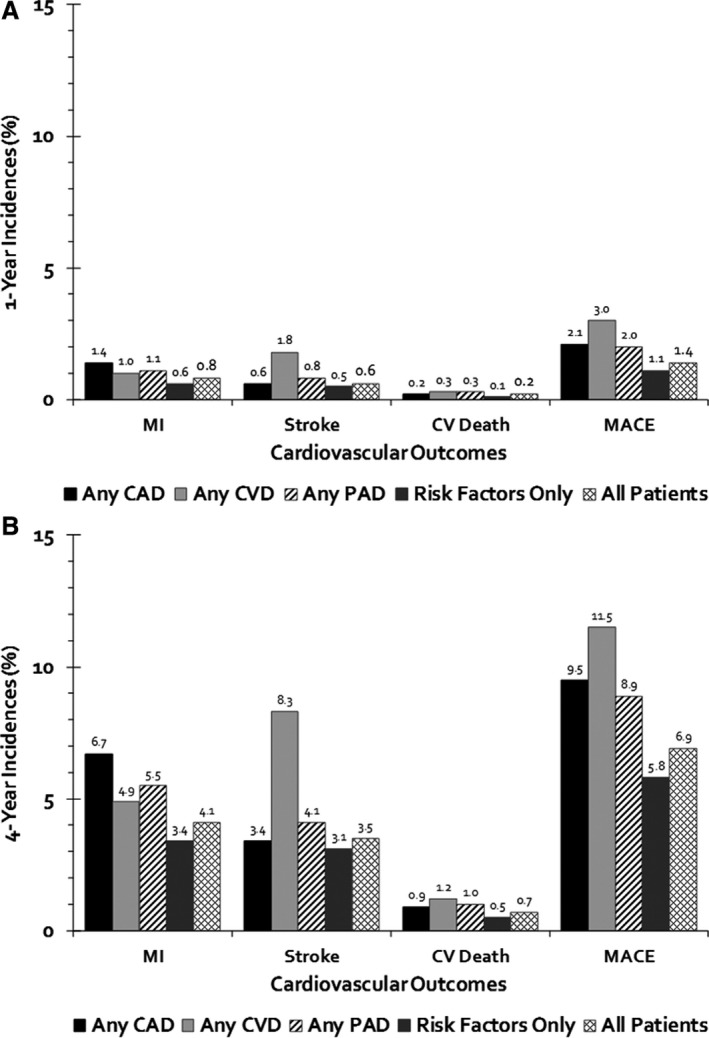
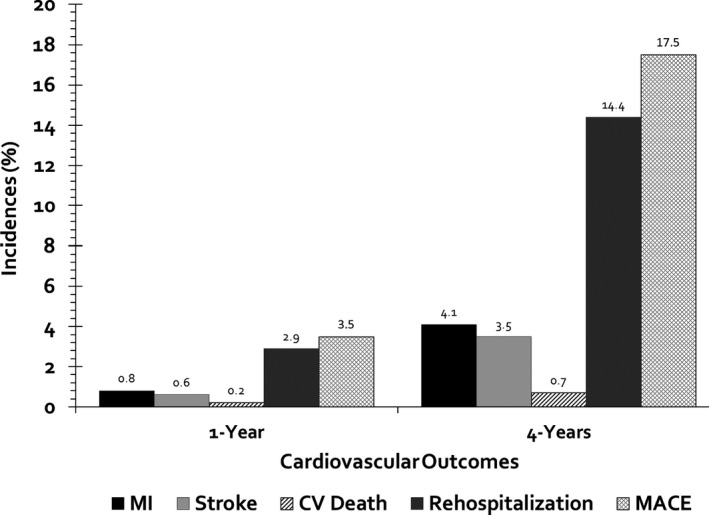
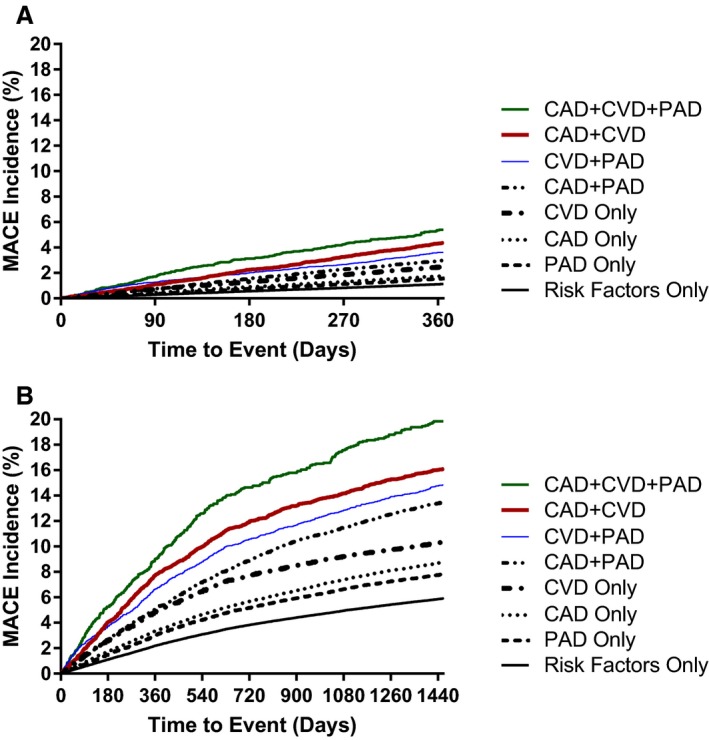
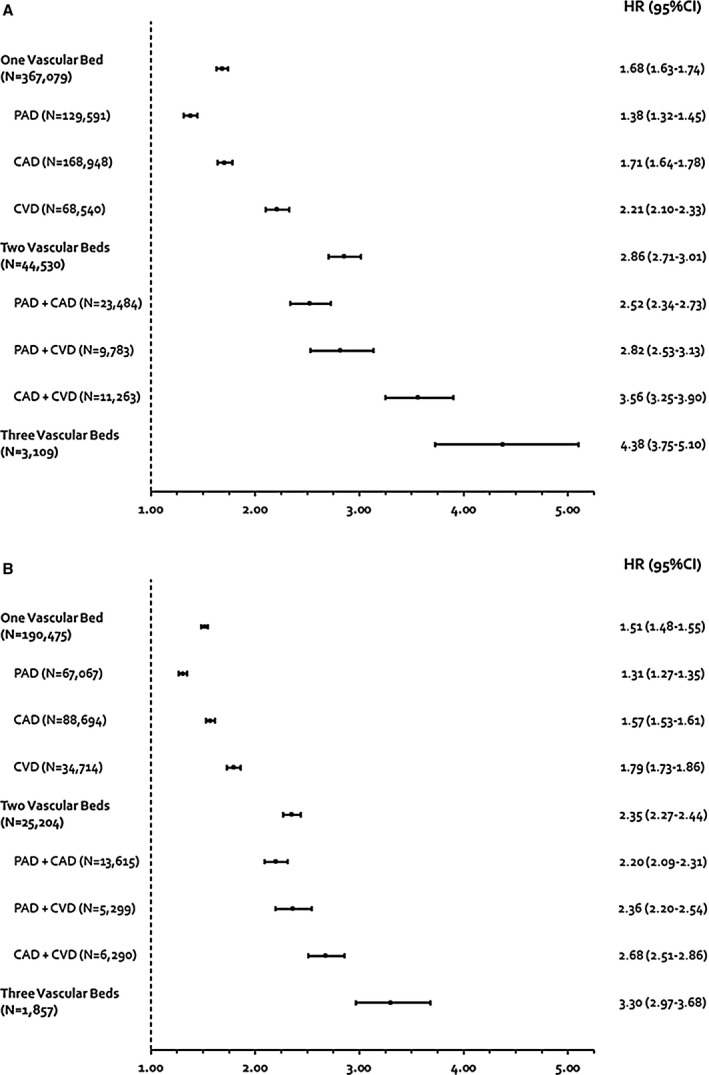
Background There is a paucity of contemporary data estimating the incidence of major adverse cardiovascular events (MACE) in patients with established atherosclerotic disease or multiple risk factors managed in routine practice. We estimated 1- and 4-year incidences of MACE and the association between MACE and vascular beds affected in these patients. Methods and Results Using US IBM MarketScan data from January 1, 2013 to December 31, 2017, we identified patients ≥45 years old with established coronary artery disease, cerebrovascular disease, peripheral artery disease, or the presence of ≥3 risk factors for atherosclerosis during 2013 with a minimum of 4 years of follow-up. We calculated 1- and 4-year incidences of MACE (cardiovascular death or hospitalization for myocardial infarction or ischemic stroke). A Cox proportional hazards regression model adjusted for age and sex was used to evaluate the association between vascular bed number/location(s) affected and MACE. We identified 1 302 856 patients with established atherosclerotic disease or risk factors for atherosclerosis. Coronary artery disease was present in 16.9% of patients, cerebrovascular disease in 7.6%, peripheral artery disease in 13.6%, and risk factors for atherosclerosis only in 66.0%. The 1- and 4-year incidences of MACE were 1.4% and 6.9%, respectively. At 4 years, MACE was more frequent in patients with atherosclerotic disease in a single (hazard ratio=1.51, 95% CI=1.48-1.55), 2-(hazard ratio=2.35, 95% CI=2.27-2.44), or all 3 vascular beds (hazard ratio=3.30, 95% CI=2.97-3.68) compared with having risk factors for atherosclerosis. Conclusions Patients with established atherosclerotic disease or who have multiple risk factors and are treated in contemporary, routine practice carry a substantial risk for MACE at 1- and 4- years of follow-up. MACE risk was shown to vary based on the number and location of vascular beds involved.
Keywords: cerebrovascular disease; coronary artery disease; established atherosclerotic disease; major adverse cardiovascular events; peripheral artery disease; risk factors.
Figures
References
-
- Heron M. Deaths: leading causes for 2015. Natl Vital Stat Rep. 2017;66:1–76. - PubMed
-
- Bhatt DL, Eagle KA, Ohman EM, Hirsch AT, Goto S, Mahoney EM, Wilson PW, Alberts MJ, D'Agostino R, Liau CS, Mas JL, Röther J, Smith SC Jr, Salette G, Contant CF, Massaro JM, Steg PG; REACH Registry Investigators . Comparative determinants of 4‐year cardiovascular event rates in stable outpatients at risk of or with atherothrombosis. JAMA. 2010;304:1350–1357. - PubMed
-
- Steg PG, Bhatt DL, Wilson PW, D'Agostino R Sr, Ohman EM, Röther J, Liau CS, Hirsch AT, Mas JL, Ikeda Y, Pencina MJ, Goto S; REACH Registry Investigators . One‐year cardiovascular event rates in outpatients with atherothrombosis. JAMA. 2007;297:1197–1206. - PubMed
-
- IBM Watson Health . White Paper: IBM MarketScan Research Databases for Health Services Researchers. April 2019. Available at: https://www.ibm.com/downloads/cas/6KNYVVQ2. Accessed November 21, 2019.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
