

Early Recognition of Burn- and Trauma-Related Acute Kidney Injury: A Pilot Comparison of Machine Learning Techniques
- PMID: 31937795
- PMCID: PMC6959341
- DOI: 10.1038/s41598-019-57083-6
Early Recognition of Burn- and Trauma-Related Acute Kidney Injury: A Pilot Comparison of Machine Learning Techniques
Abstract
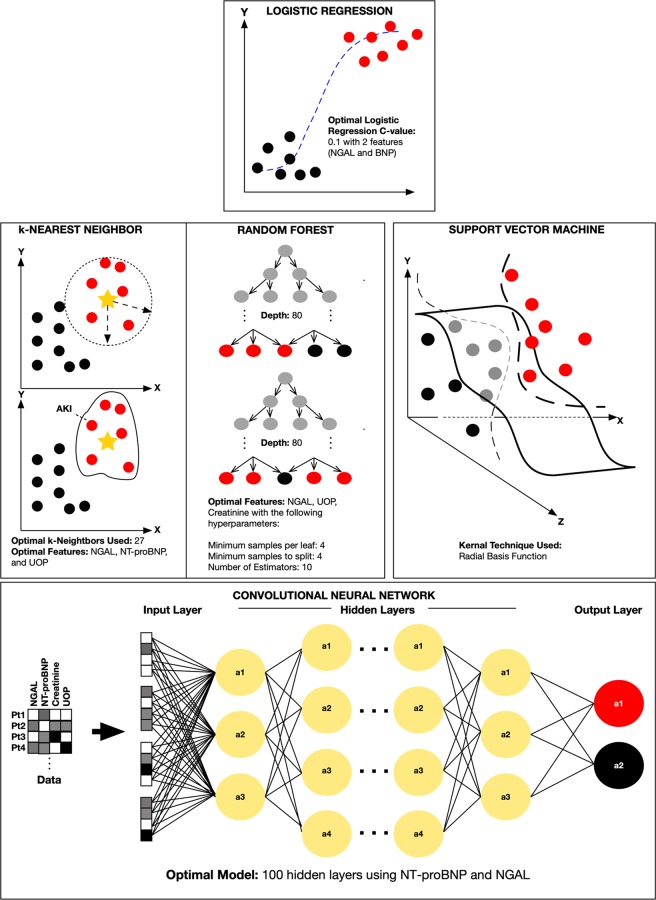
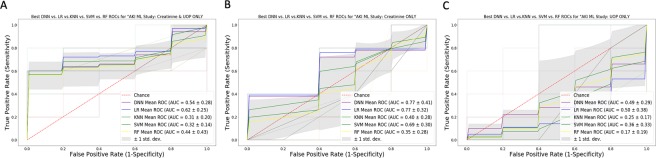
Severely burned and non-burned trauma patients are at risk for acute kidney injury (AKI). The study objective was to assess the theoretical performance of artificial intelligence (AI)/machine learning (ML) algorithms to augment AKI recognition using the novel biomarker, neutrophil gelatinase associated lipocalin (NGAL), combined with contemporary biomarkers such as N-terminal pro B-type natriuretic peptide (NT-proBNP), urine output (UOP), and plasma creatinine. Machine learning approaches including logistic regression (LR), k-nearest neighbor (k-NN), support vector machine (SVM), random forest (RF), and deep neural networks (DNN) were used in this study. The AI/ML algorithm helped predict AKI 61.8 (32.5) hours faster than the Kidney Disease and Improving Global Disease Outcomes (KDIGO) criteria for burn and non-burned trauma patients. NGAL was analytically superior to traditional AKI biomarkers such as creatinine and UOP. With ML, the AKI predictive capability of NGAL was further enhanced when combined with NT-proBNP or creatinine. The use of AI/ML could be employed with NGAL to accelerate detection of AKI in at-risk burn and non-burned trauma patients.
Conflict of interest statement
The authors declare no competing interests.
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
