

Risk modifiers of acute respiratory distress syndrome in patients with non-pulmonary sepsis: a retrospective analysis of the FORECAST study
- PMID: 31938547
- PMCID: PMC6954566
- DOI: 10.1186/s40560-020-0426-9
Risk modifiers of acute respiratory distress syndrome in patients with non-pulmonary sepsis: a retrospective analysis of the FORECAST study
Abstract
Background: Predisposing conditions and risk modifiers instead of causes and risk factors have recently been used as alternatives to identify patients at a risk of acute respiratory distress syndrome (ARDS). However, data regarding risk modifiers among patients with non-pulmonary sepsis is rare.
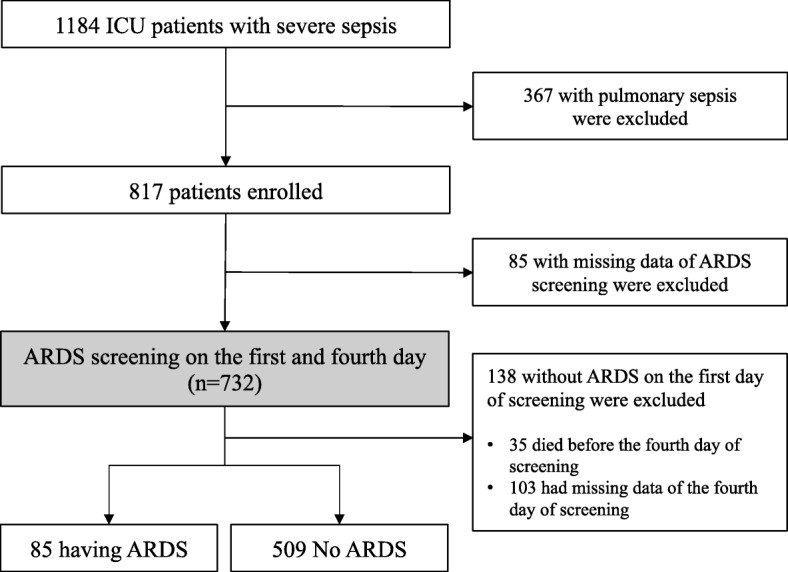
Methods: We conducted a secondary analysis of the multicenter, prospective, Focused Outcomes Research in Emergency Care in Acute Respiratory Distress Syndrome, Sepsis and Trauma (FORECAST) cohort study that was conducted in 59 intensive care units (ICUs) in Japan during January 2016-March 2017. Adult patients with severe sepsis caused by non-pulmonary infection were included, and the primary outcome was having ARDS, defined as meeting the Berlin definition on the first or fourth day of screening. Multivariate logistic regression modeling was used to identify risk modifiers associated with ARDS, and odds ratios (ORs) and their 95% confidence intervals were reported. The following explanatory variables were then assessed: age, sex, admission source, body mass index, smoking status, congestive heart failure, chronic obstructive pulmonary disease, diabetes mellitus, steroid use, statin use, infection site, septic shock, and acute physiology and chronic health evaluation (APACHE) II score.
Results: After applying inclusion and exclusion criteria, 594 patients with non-pulmonary sepsis were enrolled, among whom 85 (14.3%) had ARDS. Septic shock was diagnosed in 80% of patients with ARDS and 66% of those without ARDS (p = 0.01). APACHE II scores were higher in patients with ARDS [26 (22-33)] than in those without ARDS [21 (16-28), p < 0.01]. In the multivariate logistic regression model, the following were independently associated with ARDS: ICU admission source [OR, 1.89 (1.06-3.40) for emergency department compared with hospital wards], smoking status [OR, 0.18 (0.06-0.59) for current smoking compared with never smoked], infection site [OR, 2.39 (1.04-5.40) for soft tissue infection compared with abdominal infection], and APACHE II score [OR, 1.08 (1.05-1.12) for higher compared with lower score].
Conclusions: Soft tissue infection, ICU admission from an emergency department, and a higher APACHE II score appear to be the risk modifiers of ARDS in patients with non-pulmonary sepsis.
Keywords: Acute respiratory distress syndrome; acute respiratory failure; sepsis.
© The Author(s). 2020.
Conflict of interest statement
Competing interestsThe authors declare that they have no competing interests.
Figures
References
-
- Acute Respiratory Distress Syndrome Network. Brower RG, Matthay MA, Morris A, Schoenfeld D, Thompson BT, et al. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342:1301–1308. doi: 10.1056/NEJM200005043421801. - DOI - PubMed
-
- National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network. Wiedemann HP, Wheeler AP, Bernard GR, Thompson BT, Hayden D, et al. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med. 2006;354:2564–2575. doi: 10.1056/NEJMoa062200. - DOI - PubMed
LinkOut - more resources
Full Text Sources
