

Acute stroke and TIA patients have specific polygraphic features of obstructive sleep apnea
- PMID: 31938989
- PMCID: PMC7679322
- DOI: 10.1007/s11325-019-02010-2
Acute stroke and TIA patients have specific polygraphic features of obstructive sleep apnea
Abstract
Purpose: Obstructive sleep apnea (OSA) is associated with increased risk for stroke, which is known to further impair respiratory functions. However, it is unknown whether the type and severity of respiratory events are linked to stroke or transient ischemic attack (TIA). Thus, we investigate whether the characteristics of individual respiratory events differ between patients experiencing TIA or acute ischemic stroke and matched patients with clinically suspected sleep-disordered breathing.
Methods: Polygraphic data of 77 in-patients with acute ischemic stroke (n = 49) or TIA (n = 28) were compared to age, gender, and BMI-matched patients with suspected sleep-disordered breathing and no cerebrovascular disease. Along with conventional diagnostic parameters (e.g., apnea-hypopnea index), durations and severities of individual apneas, hypopneas and desaturations were compared between the groups separately for ischemic stroke and TIA patients.
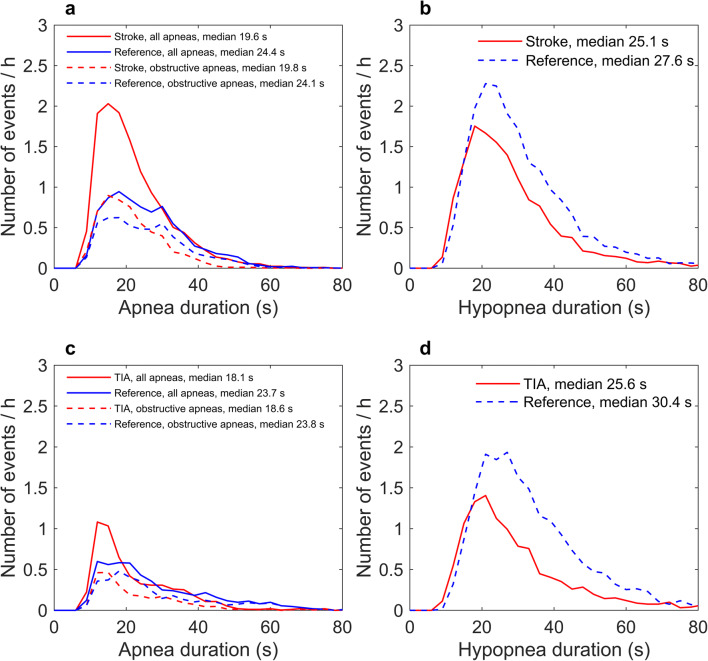
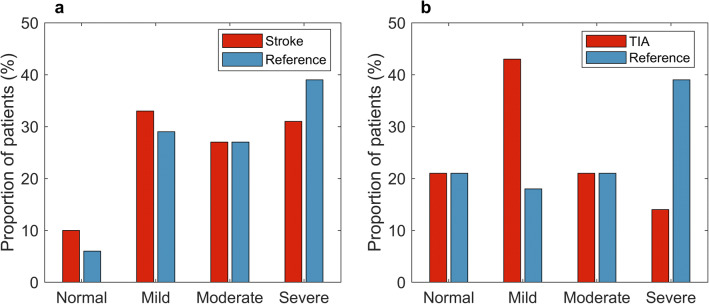
Results: Stroke and TIA patients had significantly shorter apneas and hypopneas (p < 0.001) compared to matched reference patients. Furthermore, stroke patients had more central apnea events (p = 0.007) and a trend for higher apnea/hypopnea number ratios (p = 0.091). The prevalence of OSA (apnea-hypopnea index ≥ 5) was 90% in acute stroke patients and 79% in transient ischemic attack patients.
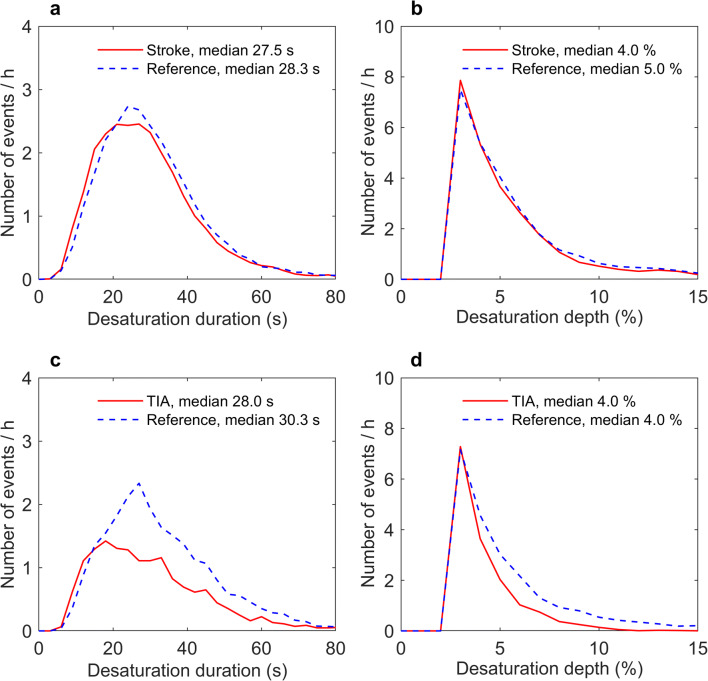
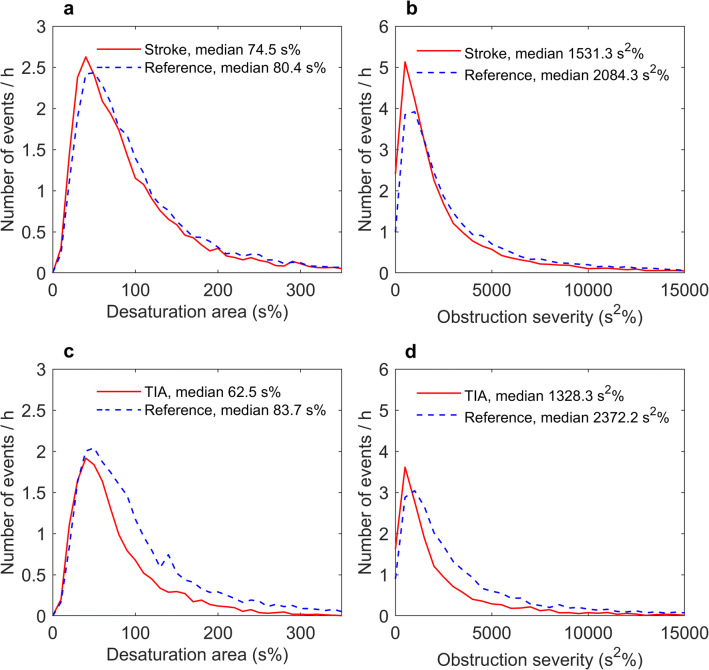
Conclusion: Stroke patients had different characteristics of respiratory events, i.e., their polygraphic phenotype of OSA differs compared to matched reference patients. The observed differences in polygraphic features might indicate that stroke and TIA patients suffer from OSA phenotype recently associated with increased cardiovascular mortality. Therefore, optimal diagnostics and treatment require routine OSA screening in patients with acute cerebrovascular disease, even without previous suspicion of OSA.
Keywords: Apnea-hypopnea index; Severity estimation; Sleep apnea; Stroke; Transient ischemic attack.
Conflict of interest statement
Dr. Kantanen has received a speaker’s honoraria from Orion, Boehringer Ingelheim, MSD, BMS.
Figures
References
-
- Redline S, Yenokyan G, Gottlieb D, Shahar E, O'Connor G, Resnick H, Diener-West M, Sanders M, Wolf P, Geraghty E, Ali T, Lebowitz M, Punjabi N. Obstructive sleep apnea-hypopnea and incident stroke: the sleep heart health study. Am J Respir Crit Care Med. 2010;182:269–277. doi: 10.1164/rccm.200911-1746OC. - DOI - PMC - PubMed
MeSH terms
Grants and funding
- 313697/Academy of Finland
- 5041767/The Research Committee of the Kuopio University Hospital Catchment Area for the State Research Funding
- 5041768/The Research Committee of the Kuopio University Hospital Catchment Area for the State Research Funding
- 5041776/The Research Committee of the Kuopio University Hospital Catchment Area for the State Research Funding
- 5041748/The Research Committee of the Kuopio University Hospital Catchment Area for the State Research Funding
LinkOut - more resources
Full Text Sources
Medical
