

Association of Clinical Outcomes With Left Ventricular Assist Device Use by Bridge to Transplant or Destination Therapy Intent: The Multicenter Study of MagLev Technology in Patients Undergoing Mechanical Circulatory Support Therapy With HeartMate 3 (MOMENTUM 3) Randomized Clinical Trial
- PMID: 31939996
- PMCID: PMC6990746
- DOI: 10.1001/jamacardio.2019.5323
Association of Clinical Outcomes With Left Ventricular Assist Device Use by Bridge to Transplant or Destination Therapy Intent: The Multicenter Study of MagLev Technology in Patients Undergoing Mechanical Circulatory Support Therapy With HeartMate 3 (MOMENTUM 3) Randomized Clinical Trial
Abstract
Importance: Left ventricular assist devices (LVADs) are well established in the treatment of advanced heart failure, but it is unclear whether outcomes are different based on the intended goal of therapy in patients who are eligible vs ineligible for heart transplant.
Objective: To determine whether clinical outcomes in the Multicenter Study of MagLev Technology in Patients Undergoing Mechanical Circulatory Support Therapy With HeartMate 3 (MOMENTUM 3) trial differed by preoperative categories of bridge to transplant (BTT) or bridge to transplant candidacy (BTC) vs destination therapy (DT).
Design, setting, and participants: This study was a prespecified secondary analysis of the MOMENTUM 3 trial, a multicenter randomized clinical trial comparing the magnetically levitated centrifugal-flow HeartMate 3 (HM3) LVAD to the axial-flow HeartMate II (HMII) pump. It was conducted in 69 centers with expertise in managing patients with advanced heart failure in the United States. Patients with advanced heart failure were randomized to an LVAD, irrespective of the intended goal of therapy (BTT/BTC or DT).
Main outcomes and measures: The primary end point was survival free of disabling stroke or reoperation to remove or replace a malfunctioning device at 2 years. Secondary end points included adverse events, functional status, and quality of life.
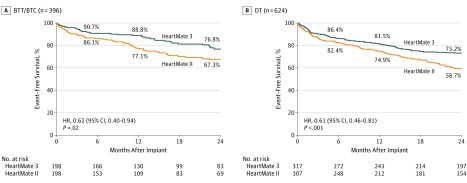
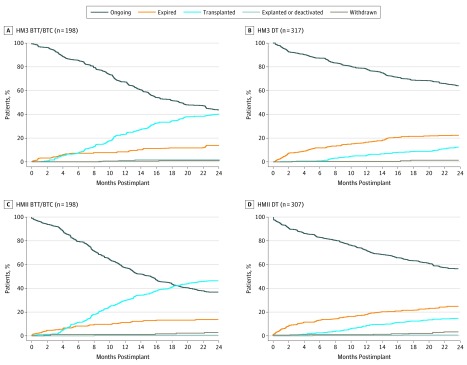
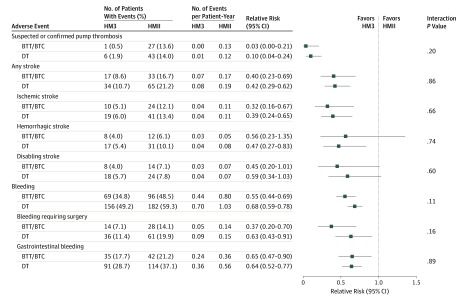
Results: Of the 1020 patients with implants (515 with HM3 devices [50.5%] and 505 with HMII devices [49.5%]), 396 (38.8%) were in the BTT/BTC group (mean [SD] age, 55 [12] years; 310 men [78.3%]) and 624 (61.2%) in the DT group (mean [SD] age, 63 [12] years; 513 men [82.2%]). Of the patients initially deemed as transplant ineligible, 84 of 624 patients (13.5%) underwent heart transplant within 2 years of LVAD implant. In the primary end point analysis, HM3 use was superior to HMII use in patients in the BTT/BTC group (76.8% vs 67.3% for survival free of disabling stroke and reoperation; hazard ratio, 0.62 [95% CI, 0.40-0.94]; log-rank P = .02) and patients in the DT group (73.2% vs 58.7%; hazard ratio, 0.61 [95% CI, 0.46-0.81]; log-rank P < .001). For patients in both BTT/BTC and DT groups, there were not significantly different reductions in rates of pump thrombosis, stroke, and gastrointestinal bleeding with HM3 use relative to HMII use. Improvements in quality of life and functional capacity for either pump were not significantly different regardless of preimplant strategy.
Conclusions and relevance: In this trial, the superior treatment effect of HM3 over HMII was similar for patients in the BTT/BTC or DT groups. It is possible that use of arbitrary categorizations based on current or future transplant eligibility should be clinically abandoned in favor of a single preimplant strategy: to extend the survival and improve the quality of life of patients with medically refractory heart failure.
Trial registration: ClinicalTrials.gov identifier: NCT02224755.
Conflict of interest statement
Figures
Comment in
-
At Last, One Indication for Left Ventricular Assist Devices-A Bridge to a Better and Longer Life.JAMA Cardiol. 2020 Mar 1;5(3):251-252. doi: 10.1001/jamacardio.2019.5592. JAMA Cardiol. 2020. PMID: 31940001 No abstract available.
-
Redefining Left Ventricular Assist Device Indications and Strategies.JAMA Cardiol. 2021 Jan 1;6(1):119-120. doi: 10.1001/jamacardio.2020.4320. JAMA Cardiol. 2021. PMID: 32965462 No abstract available.
-
Redefining Left Ventricular Assist Device Indications and Strategies-Reply.JAMA Cardiol. 2021 Jan 1;6(1):120-121. doi: 10.1001/jamacardio.2020.4323. JAMA Cardiol. 2021. PMID: 32965468 No abstract available.
-
Redefining Left Ventricular Assist Device Indications and Strategies.JAMA Cardiol. 2021 Jan 1;6(1):119. doi: 10.1001/jamacardio.2020.4303. JAMA Cardiol. 2021. PMID: 32965487 No abstract available.
References
-
- McCarthy PM, James KB, Savage RM, et al. ; Implantable LVAD Study Group . Implantable left ventricular assist device: approaching an alternative for end-stage heart failure. Circulation. 1994;90(5, pt 2):II83-II86. - PubMed
-
- Rose EA, Gelijns AC, Moskowitz AJ, et al. ; Randomized Evaluation of Mechanical Assistance for the Treatment of Congestive Heart Failure (REMATCH) Study Group . Long-term use of a left ventricular assist device for end-stage heart failure. N Engl J Med. 2001;345(20):1435-1443. doi: 10.1056/NEJMoa012175 - DOI - PubMed
