

A Multicenter Cross-Sectional Study and Systematic Review of Necrobiotic Xanthogranuloma With Proposed Diagnostic Criteria
- PMID: 31940000
- PMCID: PMC6990734
- DOI: 10.1001/jamadermatol.2019.4221
A Multicenter Cross-Sectional Study and Systematic Review of Necrobiotic Xanthogranuloma With Proposed Diagnostic Criteria
Abstract
Importance: Necrobiotic xanthogranuloma (NXG) is a non-Langerhans cell histiocytosis classically associated with paraproteinemia attributable to plasma-cell dyscrasias or lymphoproliferative disorders. Despite the morbidity of NXG, the literature is limited to case reports and small studies, and diagnostic criteria are lacking.
Objective: To evaluate the characteristics of NXG and propose diagnostic criteria.
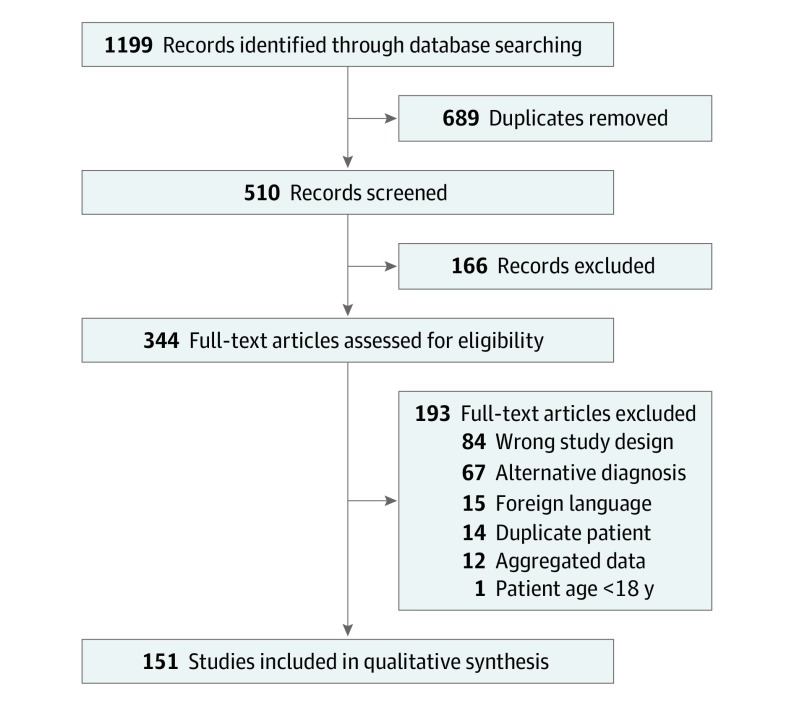
Design, setting, and participants: This multicenter cross-sectional study was conducted at tertiary academic referral centers and followed by a systematic review and a consensus exercise. The multicenter cohort included patients with NXG diagnosed at the Brigham and Women's and Massachusetts General Hospitals (2000-2018), the University of Iowa Hospitals and Clinics (2000-2018), and the University of Pennsylvania Health System (2008-2018). The systematic review was conducted in 2018 and included patients with NXG identified in the Cochrane, Ovid EMBASE, PubMed, and Web of Science databases. The consensus exercise was conducted by 8 board-certified dermatologists to identify diagnostic criteria.
Main outcomes and measures: Demographic factors, comorbidities, clinical features, and treatment response.
Results: Of 235 included patients with NXG (34 from the multicenter cohort and 201 from the systematic review results), the mean (SD) age at presentation was 61.6 (14.2) years; 147 (62.6%) were female. Paraproteinemia was detected in 193 patients (82.1%), most often IgG-κ (117 patients [50.0%]). A malignant condition was detected in 59 patients (25.1%), most often multiple myeloma (33 patients [14.0%]). The overall rate of paraproteinemia and/or a malignant condition was 83.8% (197 patients). In the multicenter cohort, evolution of paraproteinemia into multiple myeloma was observed up to 5.7 years (median [range], 2.4 [0.1-5.7] years) after NXG presentation. Cutaneous lesions consisted of papules, plaques, and/or nodules, typically yellow or orange in color (113 of 187 [60.4%]) with a periorbital distribution (130 of 219 [59.3%]). The eye was the leading site of extracutaneous involvement (34 of 235 [14.5%]). In the multicenter cohort, intravenous immunoglobulin had the best treatment response rate (9 of 9 patients [100%]), followed by antimalarial drugs (4 of 5 patients [80%]), intralesional triamcinolone (6 of 8 patients [75%]), surgery (3 of 4 patients [75%]), chemotherapy (8 of 12 patients [67%]), and lenalidomide or thalidomide (5 of 8 patients [63%]). The consensus exercise yielded 2 major criteria, which were (1) clinical and (2) histopathological features consistent with NXG, and 2 minor criteria, consisting of (1) paraproteinemia, plasma-cell dyscrasia, and/or other associated lymphoproliferative disorder and (2) periorbital distribution of cutaneous lesions. In the absence of foreign body, infection, or another identifiable cause, fulfillment of both major and at least 1 minor criterion were proposed to establish the diagnosis of NXG.
Conclusions and relevance: Necrobiotic xanthogranuloma is a multisystem disorder associated with paraproteinemia and malignant conditions. The proposed diagnostic criteria may advance clinical research and should be validated.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
