

Interventions and Operations 5 Years After Bariatric Surgery in a Cohort From the US National Patient-Centered Clinical Research Network Bariatric Study
- PMID: 31940024
- PMCID: PMC6990709
- DOI: 10.1001/jamasurg.2019.5470
Interventions and Operations 5 Years After Bariatric Surgery in a Cohort From the US National Patient-Centered Clinical Research Network Bariatric Study
Abstract
Importance: Additional data comparing longer-term problems associated with various bariatric surgical procedures are needed for shared decision-making.
Objective: To compare the risks of intervention, operation, endoscopy, hospitalization, and mortality up to 5 years after 2 bariatric surgical procedures.
Design, setting, and participants: Adults who underwent Roux-en-Y gastric bypass (RYGB) or sleeve gastrectomy (SG) between January 1, 2005, and September 30, 2015, within the National Patient-Centered Clinical Research Network. Data from 33 560 adults at 10 centers within 4 clinical data research networks were included in this cohort study. Information was extracted from electronic health records using a common data model and linked to insurance claims and mortality indices. Analyses were conducted from January 2018 through October 2019.
Exposures: Bariatric surgical procedures.
Main outcomes and measures: The primary outcome was time until operation or intervention. Secondary outcomes included endoscopy, hospitalization, and mortality rates.
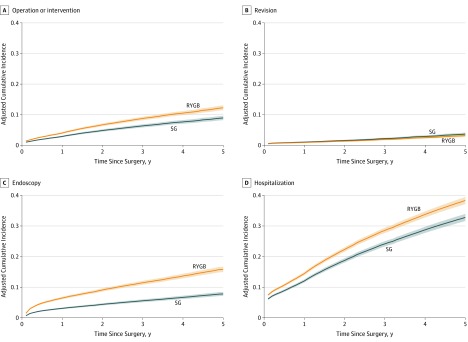
Results: Of 33 560 adults, 18 056 (54%) underwent RYGB, and 15 504 (46%) underwent SG. The median (interquartile range) follow-up for operation or intervention was 3.4 (1.6-5.0) years for RYGB and 2.2 (0.9-3.6) years for SG. The overall mean (SD) patient age was 45.0 (11.5) years, and the overall mean (SD) patient body mass index was 49.1 (7.9). The cohort was composed predominantly of women (80%) and white individuals (66%), with 26% of Hispanic ethnicity. Operation or intervention was less likely for SG than for RYGB (hazard ratio, 0.72; 95% CI, 0.65-0.79; P < .001). The estimated, adjusted cumulative incidence rates of operation or intervention at 5 years were 8.94% (95% CI, 8.23%-9.65%) for SG and 12.27% (95% CI, 11.49%-13.05%) for RYGB. Hospitalization was less likely for SG than for RYGB (hazard ratio, 0.82; 95% CI, 0.78-0.87; P < .001), and the 5-year adjusted cumulative incidence rates were 32.79% (95% CI, 31.62%-33.94%) for SG and 38.33% (95% CI, 37.17%-39.46%) for RYGB. Endoscopy was less likely for SG than for RYGB (hazard ratio, 0.47; 95% CI, 0.43-0.52; P < .001), and the adjusted cumulative incidence rates at 5 years were 7.80% (95% CI, 7.15%-8.43%) for SG and 15.83% (95% CI, 14.94%-16.71%) for RYGB. There were no differences in all-cause mortality between SG and RYGB.
Conclusions and relevance: Interventions, operations, and hospitalizations were relatively common after bariatric surgical procedures and were more often associated with RYGB than SG.
Trial registration: ClinicalTrials.gov identifier: NCT02741674.
Conflict of interest statement
Figures
Comment in
-
Bariatric Surgery Is Safe and It Works.JAMA Surg. 2020 Mar 1;155(3):205. doi: 10.1001/jamasurg.2019.5471. JAMA Surg. 2020. PMID: 31940018 No abstract available.
-
Evidence-Based and Patient-Centered Decisions Regarding Bariatric Surgery-Reply.JAMA Surg. 2020 Sep 1;155(9):902-903. doi: 10.1001/jamasurg.2020.1530. JAMA Surg. 2020. PMID: 32609309 No abstract available.
-
Evidence-Based and Patient-Centered Decisions Regarding Bariatric Surgery.JAMA Surg. 2020 Sep 1;155(9):902. doi: 10.1001/jamasurg.2020.1524. JAMA Surg. 2020. PMID: 32609311 No abstract available.
References
-
- Hutter MM, Schirmer BD, Jones DB, et al. . First report from the American College of Surgeons Bariatric Surgery Center Network: laparoscopic sleeve gastrectomy has morbidity and effectiveness positioned between the band and the bypass. Ann Surg. 2011;254(3):410-420. doi:10.1097/SLA.0b013e31822c9dac - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
