

Biomarkers and clinical scores to aid the identification of disease severity and intensive care requirement following activation of an in-hospital sepsis code
- PMID: 31940096
- PMCID: PMC6962418
- DOI: 10.1186/s13613-020-0625-5
Biomarkers and clinical scores to aid the identification of disease severity and intensive care requirement following activation of an in-hospital sepsis code
Abstract
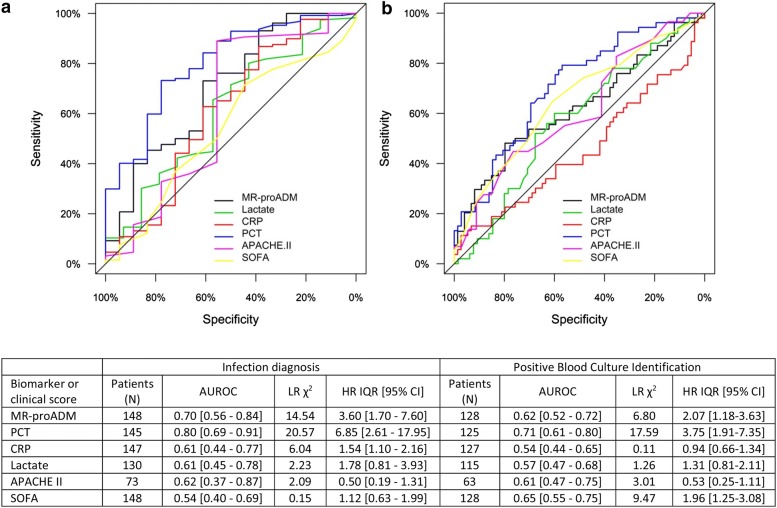
Background: Few validated biomarker or clinical score combinations exist which can discriminate between cases of infection and other non-infectious conditions following activation of an in-hospital sepsis code, as well as provide an accurate severity assessment of the corresponding host response. This study aimed to identify suitable blood biomarker (MR-proADM, PCT, CRP and lactate) or clinical score (SOFA and APACHE II) combinations to address this unmet clinical need.
Methods: A prospective, observational study of patients activating the Vall d'Hebron University Hospital sepsis code (ISC) within the emergency department (ED), hospital wards and intensive care unit (ICU). Area under the receiver operating characteristic (AUROC) curves, logistic and Cox regression analysis were used to assess performance.
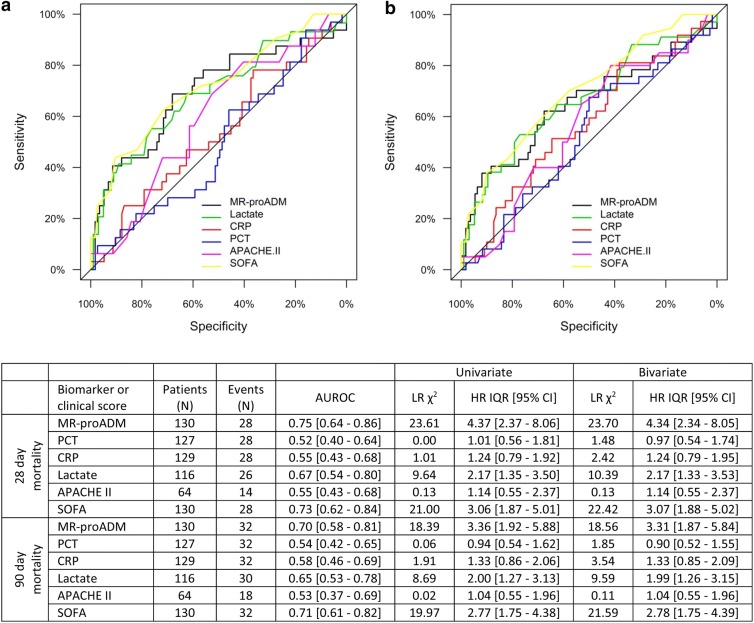
Results: 148 patients fulfilled the Vall d'Hebron ISC criteria, of which 130 (87.8%) were retrospectively found to have a confirmed diagnosis of infection. Both PCT and MR-proADM had a moderate-to-high performance in discriminating between infected and non-infected patients following ISC activation, although the optimal PCT cut-off varied significantly across departments. Similarly, MR-proADM and SOFA performed well in predicting 28- and 90-day mortality within the total infected patient population, as well as within patients presenting with a community-acquired infection or following a medical emergency or prior surgical procedure. Importantly, MR-proADM also showed a high association with the requirement for ICU admission after ED presentation [OR (95% CI) 8.18 (1.75-28.33)] or during treatment on the ward [OR (95% CI) 3.64 (1.43-9.29)], although the predictive performance of all biomarkers and clinical scores diminished between both settings.
Conclusions: Results suggest that the individual use of PCT and MR-proADM might help to accurately identify patients with infection and assess the overall severity of the host response, respectively. In addition, the use of MR-proADM could accurately identify patients requiring admission onto the ICU, irrespective of whether patients presented to the ED or were undergoing treatment on the ward. Initial measurement of both biomarkers might therefore facilitate early treatment strategies following activation of an in-hospital sepsis code.
Conflict of interest statement
All authors have provided information on potential conflicts of interests directly or indirectly related to the work submitted in the journal’s disclosure forms. The authors declare that they have no competing interests.
Figures
References
-
- Elke G, Bloos F, Wilson DC, Brunkhorst FM, Briegel J, Reinhart K, et al. The use of mid-regional proadrenomedullin to identify disease severity and treatment response to sepsis—a secondary analysis of a large randomised controlled trial. Crit Care. 2018;22(1):79. doi: 10.1186/s13054-018-2001-5. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
