

A Randomized Trial of Erythropoietin for Neuroprotection in Preterm Infants
- PMID: 31940698
- PMCID: PMC7060076
- DOI: 10.1056/NEJMoa1907423
A Randomized Trial of Erythropoietin for Neuroprotection in Preterm Infants
Abstract
Background: High-dose erythropoietin has been shown to have a neuroprotective effect in preclinical models of neonatal brain injury, and phase 2 trials have suggested possible efficacy; however, the benefits and safety of this therapy in extremely preterm infants have not been established.
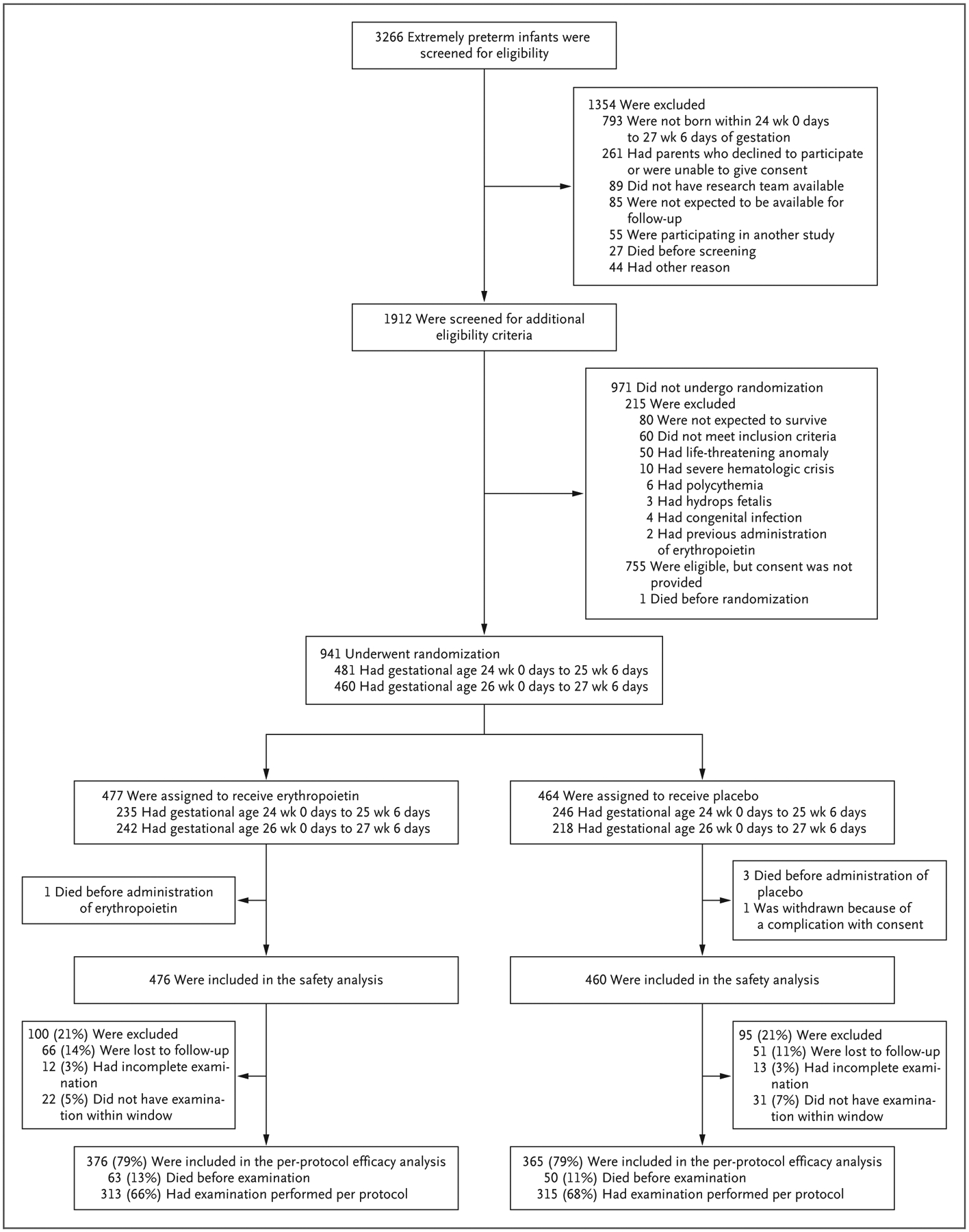
Methods: In this multicenter, randomized, double-blind trial of high-dose erythropoietin, we assigned 941 infants who were born at 24 weeks 0 days to 27 weeks 6 days of gestation to receive erythropoietin or placebo within 24 hours after birth. Erythropoietin was administered intravenously at a dose of 1000 U per kilogram of body weight every 48 hours for a total of six doses, followed by a maintenance dose of 400 U per kilogram three times per week by subcutaneous injection through 32 completed weeks of postmenstrual age. Placebo was administered as intravenous saline followed by sham injections. The primary outcome was death or severe neurodevelopmental impairment at 22 to 26 months of postmenstrual age. Severe neurodevelopmental impairment was defined as severe cerebral palsy or a composite motor or composite cognitive score of less than 70 (which corresponds to 2 SD below the mean, with higher scores indicating better performance) on the Bayley Scales of Infant and Toddler Development, third edition.
Results: A total of 741 infants were included in the per-protocol efficacy analysis: 376 received erythropoietin and 365 received placebo. There was no significant difference between the erythropoietin group and the placebo group in the incidence of death or severe neurodevelopmental impairment at 2 years of age (97 children [26%] vs. 94 children [26%]; relative risk, 1.03; 95% confidence interval, 0.81 to 1.32; P = 0.80). There were no significant differences between the groups in the rates of retinopathy of prematurity, intracranial hemorrhage, sepsis, necrotizing enterocolitis, bronchopulmonary dysplasia, or death or in the frequency of serious adverse events.
Conclusions: High-dose erythropoietin treatment administered to extremely preterm infants from 24 hours after birth through 32 weeks of postmenstrual age did not result in a lower risk of severe neurodevelopmental impairment or death at 2 years of age. (Funded by the National Institute of Neurological Disorders and Stroke; PENUT ClinicalTrials.gov number, NCT01378273.).
Copyright © 2020 Massachusetts Medical Society.
Conflict of interest statement
Dr. Hartman reports receiving consulting fees from Best Doctors. No other potential conflict of interest relevant to this article was reported.
Figures


Comment in
-
Erythropoietin in Preterm Infants.N Engl J Med. 2020 May 7;382(19):1862. doi: 10.1056/NEJMc2002493. N Engl J Med. 2020. PMID: 32374968 No abstract available.
References
-
- Matthews TJ, MacDorman MF, Thoma ME. Infant mortality statistics from the 2013 period linked birth/infant death data set. Natl Vital Stat Rep 2015; 64: 1–30. - PubMed
-
- Jarjour IT. Neurodevelopmental outcome after extreme prematurity: a review of the literature. Pediatr Neurol 2015; 52: 143–52. - PubMed
-
- Franz AP, Bolat GU, Bolat H, et al. Attention-deficit/hyperactivity disorder and very preterm/very low birth weight: a meta-analysis. Pediatrics 2018; 141(1): e20171645. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical