

Survival After Intravenous Versus Intraosseous Amiodarone, Lidocaine, or Placebo in Out-of-Hospital Shock-Refractory Cardiac Arrest
- PMID: 31941354
- PMCID: PMC7009320
- DOI: 10.1161/CIRCULATIONAHA.119.042240
Survival After Intravenous Versus Intraosseous Amiodarone, Lidocaine, or Placebo in Out-of-Hospital Shock-Refractory Cardiac Arrest
Abstract
Background: Antiarrhythmic drugs have not proven to significantly improve overall survival after out-of-hospital cardiac arrest from shock-refractory ventricular fibrillation/pulseless ventricular tachycardia. How this might be influenced by the route of drug administration is not known.
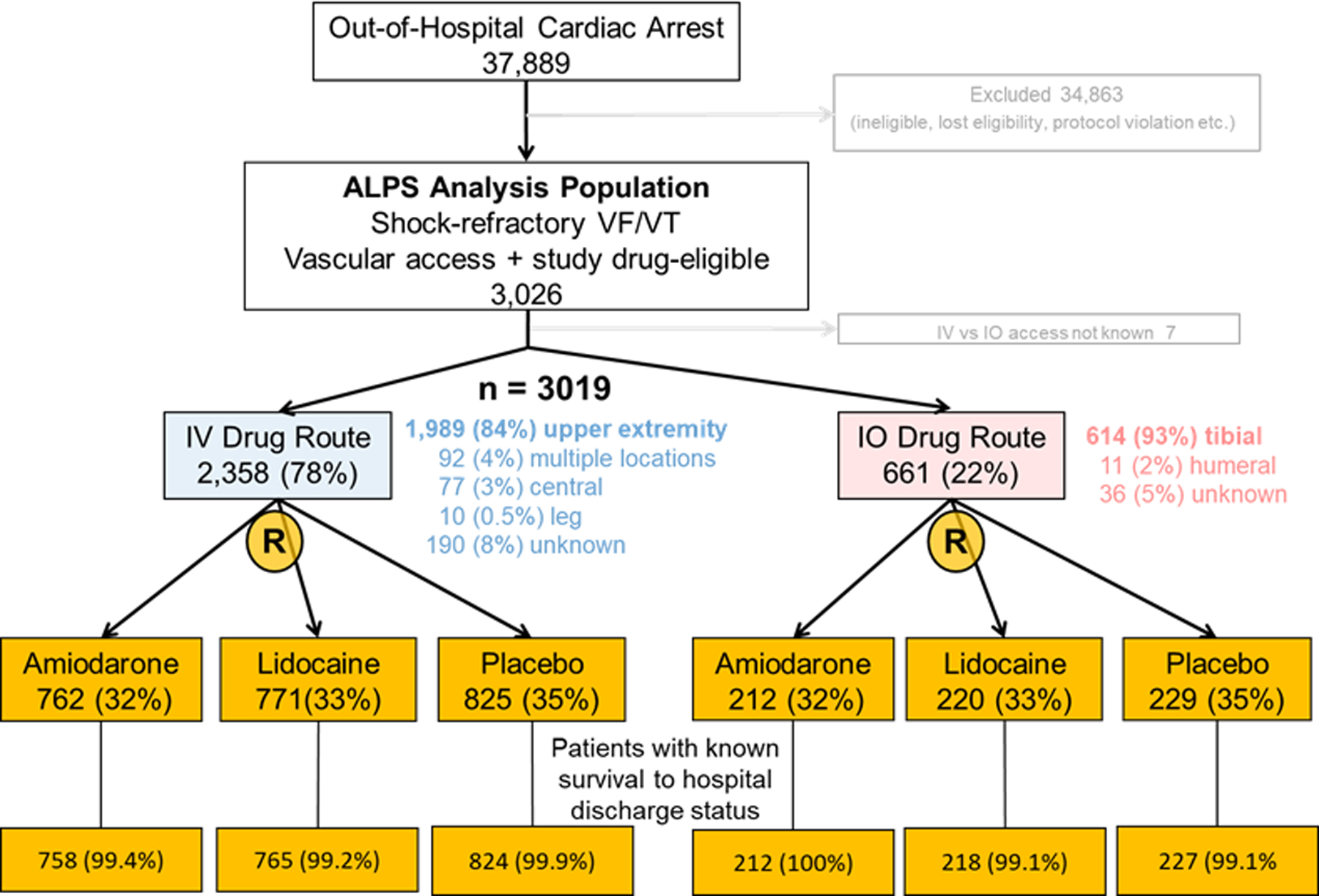
Methods: In this prespecified analysis of a randomized, placebo-controlled clinical trial, we compared the differences in survival to hospital discharge in adults with shock-refractory ventricular fibrillation/pulseless ventricular tachycardia out-of-hospital cardiac arrest who were randomly assigned by emergency medical services personnel to an antiarrhythmic drug versus placebo in the ALPS trial (Resuscitation Outcomes Consortium Amiodarone, Lidocaine or Placebo Study), when stratified by the intravenous versus intraosseous route of administration.
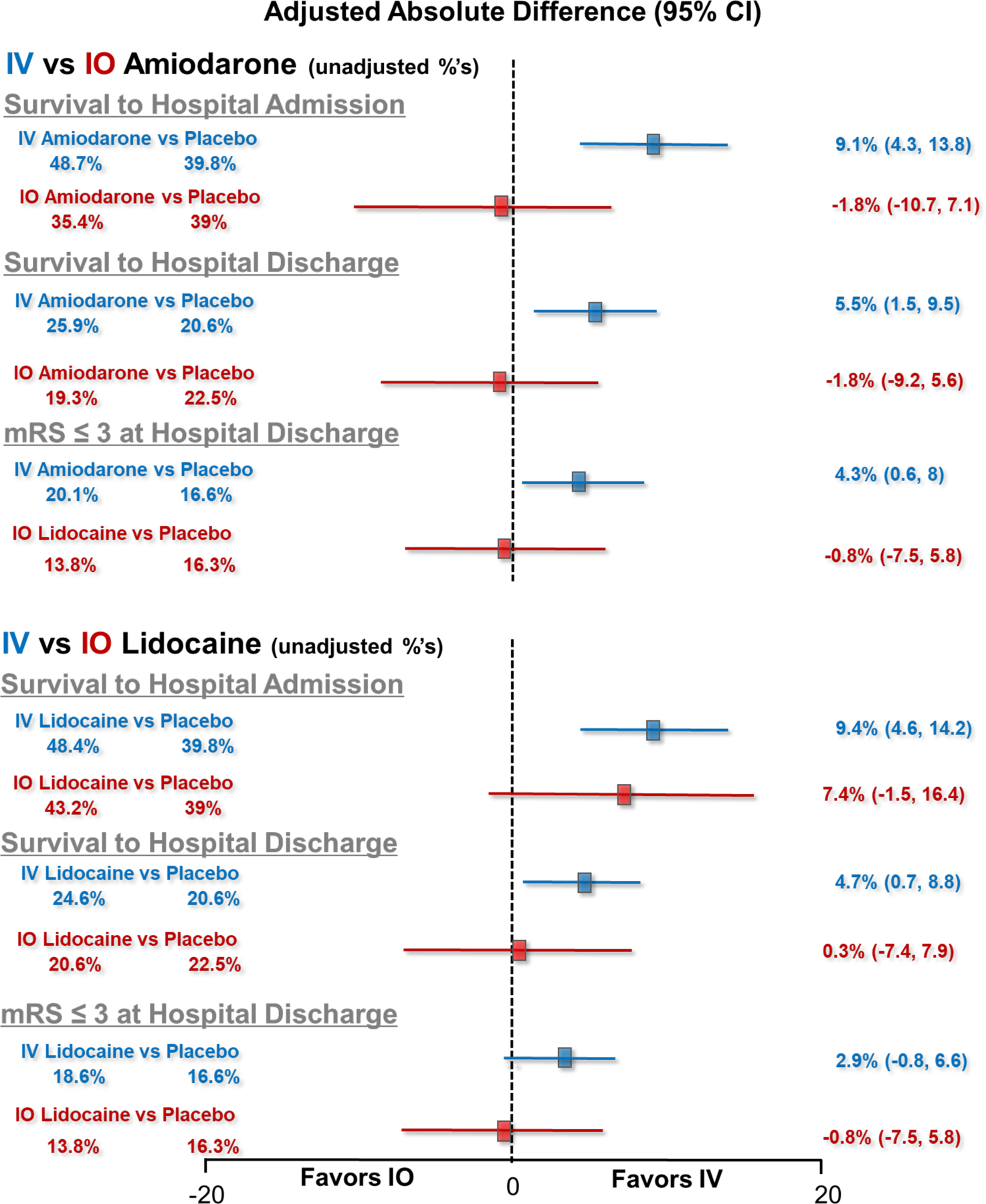
Results: Of 3019 randomly assigned patients with a known vascular access site, 2358 received ALPS drugs intravenously and 661 patients by the intraosseous route. Intraosseous and intravenous groups differed in sex, time-to-emergency medical services arrival, and some cardiopulmonary resuscitation characteristics, but were similar in others, including time-to-intravenous/intrasosseous drug receipt. Overall hospital discharge survival was 23%. In comparison with placebo, discharge survival was significantly higher in recipients of intravenous amiodarone (adjusted risk ratio, 1.26 [95% CI, 1.06-1.50]; adjusted absolute survival difference, 5.5% [95% CI, 1.5-9.5]) and intravenous lidocaine (adjusted risk ratio, 1.21 [95% CI, 1.02-1.45]; adjusted absolute survival difference, 4.7% [95% CI, 0.7-8.8]); but not in recipients of intraosseous amiodarone (adjusted risk ratio, 0.94 [95% CI, 0.66-1.32]) or intraosseous lidocaine (adjusted risk ratio, 1.03 [95% CI, 0.74-1.44]). Survival to hospital admission also increased significantly when drugs were given intravenously but not intraosseously, and favored improved neurological outcome at discharge. There were no outcome differences between intravenous and intraosseous placebo, indicating that the access route itself did not demarcate patients with poor prognosis. The study was underpowered to assess intravenous/intraosseous drug interactions, which were not statistically significant.
Conclusions: We found no significant effect modification by drug administration route for amiodarone or lidocaine in comparison with placebo during out-of-hospital cardiac arrest. However, point estimates for the effects of both drugs in comparison with placebo were significantly greater for the intravenous than for the intraosseous route across virtually all outcomes and beneficial only for the intravenous route. Given that the study was underpowered to statistically assess interactions, these findings signal the potential importance of the drug administration route during resuscitation that merits further investigation.
Keywords: amiodarone; antiarrhythmia agents; arrhythmias, cardiac; heart arrest.
Figures
References
-
- Kudenchuk PJ, Brown SP, Daya M, Rea T, Nichol G, Morrison LJ, Leroux B, Vaillancourt C, Wittwer L, Callaway CW et al. Amiodarone, lidocaine or placebo in out of hospital cardiac arrest. N Engl J Med 2016;374:1711–1722. - PubMed
-
- American Heart Association 2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Part 7.2 Management of cardiac arrest. Circulation 2005;112 (issue no. 24, suppl): IV58–IV66. - PubMed
-
- Leidel BA, Kirchhoff C, Bogner V, Stegmaier J, Mutschler W, Kanz KG, Braunstein V. Is the intraosseous access route fast and efficacious compared to conventional central venous catheterization in adult patients under resuscitation in the emergency department? Patient Saf Surg 2009;3:24. - PMC - PubMed
-
- Fuchs S, LaCovey D, Paris P. A prehospital model of intraosseous infusion. Ann Emerg Med 1991;20;371–374. - PubMed
-
- Reades R, Studnek JR, Vandeventer S, Garrett J. Intraosseous versus intravenous vascular access during out of hospital cardiac arrest: A randomized controlled trial. Ann Emerg Med 2011;58:509–16. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
