

An International Multicenter Evaluation of Type 5 Long QT Syndrome: A Low Penetrant Primary Arrhythmic Condition
- PMID: 31941373
- PMCID: PMC7035205
- DOI: 10.1161/CIRCULATIONAHA.119.043114
An International Multicenter Evaluation of Type 5 Long QT Syndrome: A Low Penetrant Primary Arrhythmic Condition
Abstract
Background: Insight into type 5 long QT syndrome (LQT5) has been limited to case reports and small family series. Improved understanding of the clinical phenotype and genetic features associated with rare KCNE1 variants implicated in LQT5 was sought through an international multicenter collaboration.
Methods: Patients with either presumed autosomal dominant LQT5 (N = 229) or the recessive Type 2 Jervell and Lange-Nielsen syndrome (N = 19) were enrolled from 22 genetic arrhythmia clinics and 4 registries from 9 countries. KCNE1 variants were evaluated for ECG penetrance (defined as QTc >460 ms on presenting ECG) and genotype-phenotype segregation. Multivariable Cox regression was used to compare the associations between clinical and genetic variables with a composite primary outcome of definite arrhythmic events, including appropriate implantable cardioverter-defibrillator shocks, aborted cardiac arrest, and sudden cardiac death.
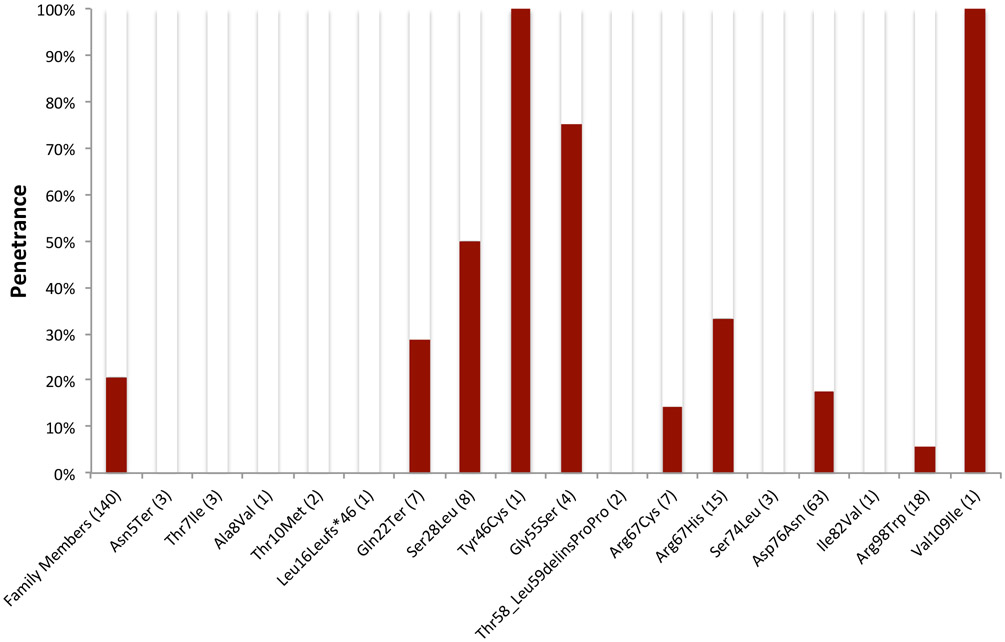
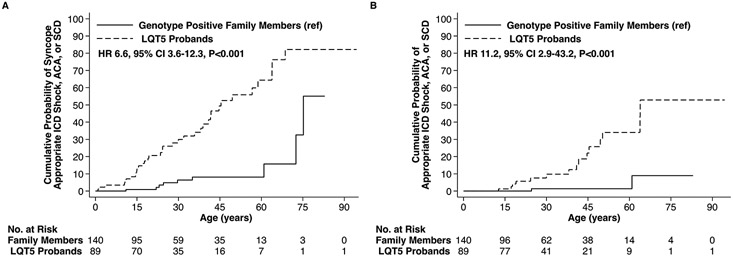
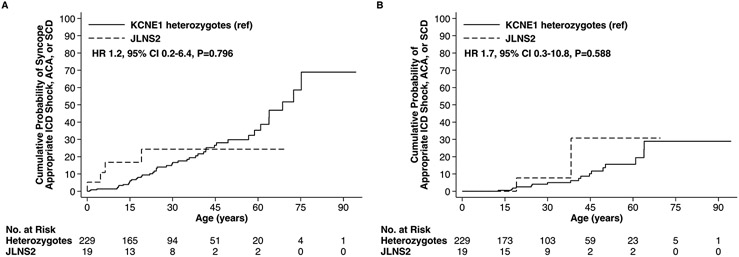
Results: A total of 32 distinct KCNE1 rare variants were identified in 89 probands and 140 genotype positive family members with presumed LQT5 and an additional 19 Type 2 Jervell and Lange-Nielsen syndrome patients. Among presumed LQT5 patients, the mean QTc on presenting ECG was significantly longer in probands (476.9±38.6 ms) compared with genotype positive family members (441.8±30.9 ms, P<0.001). ECG penetrance for heterozygous genotype positive family members was 20.7% (29/140). A definite arrhythmic event was experienced in 16.9% (15/89) of heterozygous probands in comparison with 1.4% (2/140) of family members (adjusted hazard ratio [HR] 11.6 [95% CI, 2.6-52.2]; P=0.001). Event incidence did not differ significantly for Type 2 Jervell and Lange-Nielsen syndrome patients relative to the overall heterozygous cohort (10.5% [2/19]; HR 1.7 [95% CI, 0.3-10.8], P=0.590). The cumulative prevalence of the 32 KCNE1 variants in the Genome Aggregation Database, which is a human database of exome and genome sequencing data from now over 140 000 individuals, was 238-fold greater than the anticipated prevalence of all LQT5 combined (0.238% vs 0.001%).
Conclusions: The present study suggests that putative/confirmed loss-of-function KCNE1 variants predispose to QT prolongation, however, the low ECG penetrance observed suggests they do not manifest clinically in the majority of individuals, aligning with the mild phenotype observed for Type 2 Jervell and Lange-Nielsen syndrome patients.
Keywords: arrhythmia; genetics; long QT syndrome; penetrance; sudden cardiac death.
Figures
Comment in
-
Time to Rethink the Genetic Architecture of Long QT Syndrome.Circulation. 2020 Feb 11;141(6):440-443. doi: 10.1161/CIRCULATIONAHA.119.044760. Epub 2020 Feb 10. Circulation. 2020. PMID: 32078431 No abstract available.
References
-
- Mazzanti A, Maragna R, Priori S. Genetic causes of sudden cardiac death in the young. Current Opinion in Cardiology. 2017;32:253–261. - PubMed
-
- Schwartz PJ, Ackerman MJ, Wilde AAM. Channelopathies as causes of sudden cardiac death. Card Electrophysiol Clin. 2017;9:537–549. - PubMed
-
- Sanguinetti MC, Curran ME, Zou A, Shen J, Spector PS, Atkinson DL, Keating MT. Coassembly of K(V)LQT1 and minK (IsK) proteins to form cardiac I(Ks) potassium channel. Nature. 1996;384:80–83. - PubMed
