

Pregnancy-specific malarial immunity and risk of malaria in pregnancy and adverse birth outcomes: a systematic review
- PMID: 31941488
- PMCID: PMC6964062
- DOI: 10.1186/s12916-019-1467-6
Pregnancy-specific malarial immunity and risk of malaria in pregnancy and adverse birth outcomes: a systematic review
Abstract
Background: In endemic areas, pregnant women are highly susceptible to Plasmodium falciparum malaria characterized by the accumulation of parasitized red blood cells (pRBC) in the placenta. In subsequent pregnancies, women develop protective immunity to pregnancy-associated malaria and this has been hypothesized to be due to the acquisition of antibodies to the parasite variant surface antigen VAR2CSA. In this systematic review we provide the first synthesis of the association between antibodies to pregnancy-specific P. falciparum antigens and pregnancy and birth outcomes.
Methods: We conducted a systematic review and meta-analysis of population-based studies (published up to 07 June 2019) of pregnant women living in P. falciparum endemic areas that examined antibody responses to pregnancy-specific P. falciparum antigens and outcomes including placental malaria, low birthweight, preterm birth, peripheral parasitaemia, maternal anaemia, and severe malaria.
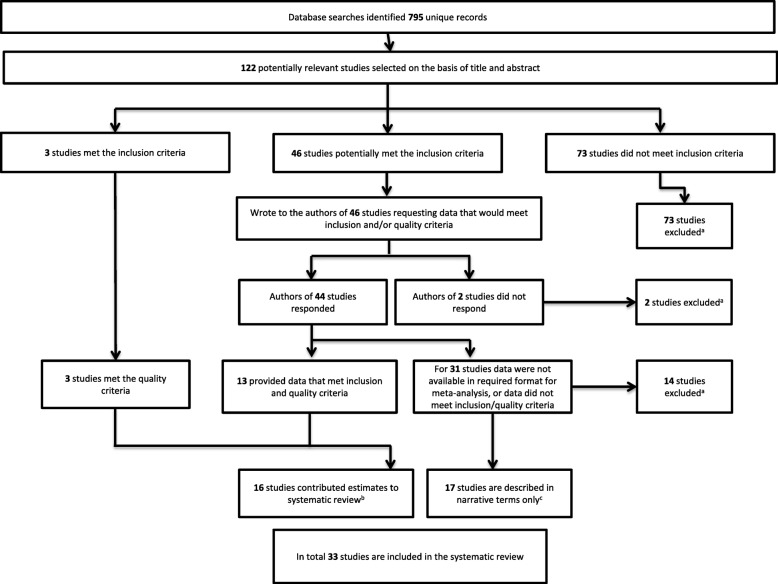
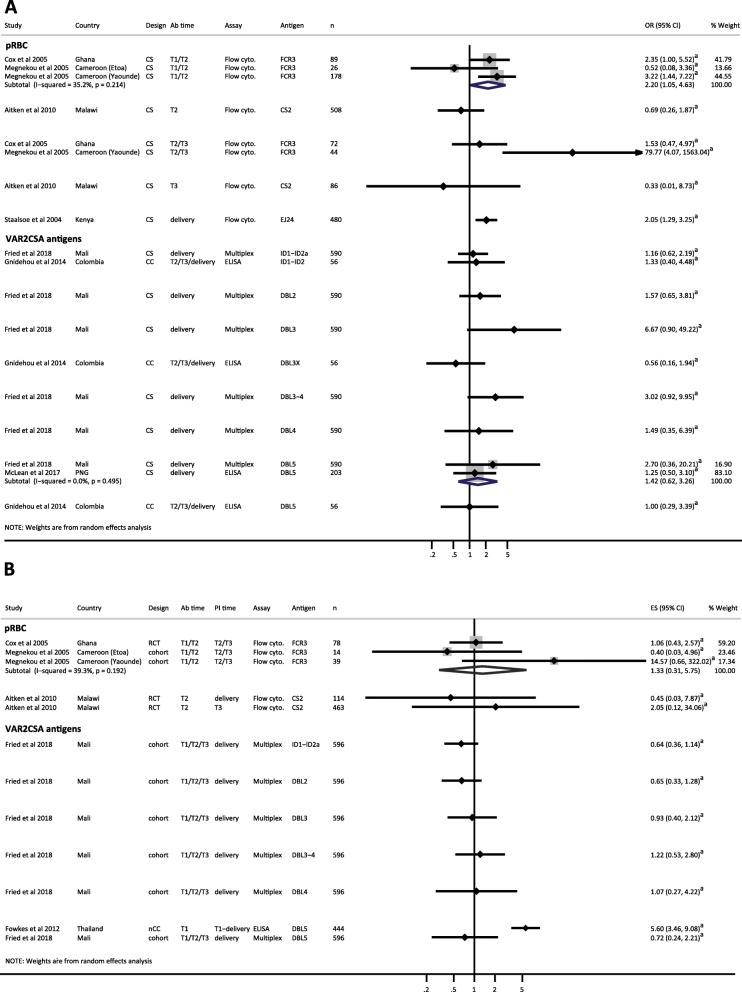
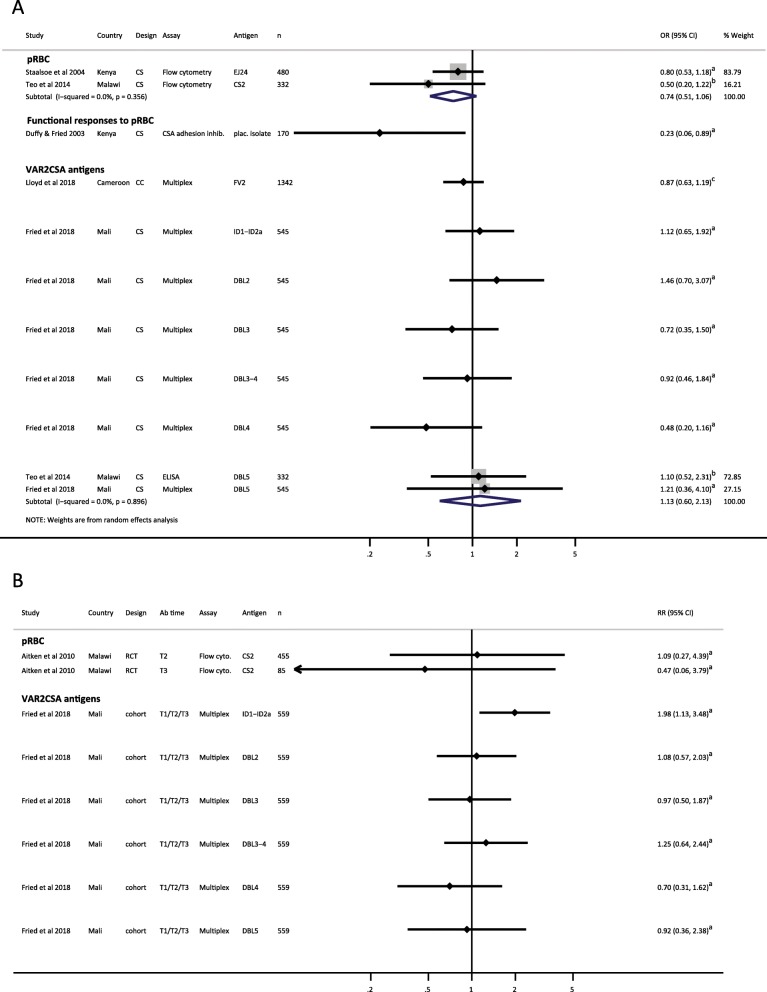
Results: We searched 6 databases and identified 33 studies (30 from Africa) that met predetermined inclusion and quality criteria: 16 studies contributed estimates in a format enabling inclusion in meta-analysis and 17 were included in narrative form only. Estimates were mostly from cross-sectional data (10 studies) and were heterogeneous in terms of magnitude and direction of effect. Included studies varied in terms of antigens tested, methodology used to measure antibody responses, and epidemiological setting. Antibody responses to pregnancy-specific pRBC and VAR2CSA antigens, measured at delivery, were associated with placental malaria (9 studies) and may therefore represent markers of infection, rather than correlates of protection. Antibody responses to pregnancy-specific pRBC, but not recombinant VAR2CSA antigens, were associated with trends towards protection from low birthweight (5 studies).
Conclusions: Whilst antibody responses to several antigens were positively associated with the presence of placental and peripheral infections, this review did not identify evidence that any specific antibody response is associated with protection from pregnancy-associated malaria across multiple populations. Further prospective cohort studies using standardized laboratory methods to examine responses to a broad range of antigens in different epidemiological settings and throughout the gestational period, will be necessary to identify and prioritize pregnancy-specific P. falciparum antigens to advance the development of vaccines and serosurveillance tools targeting pregnant women.
Keywords: Antibodies; Epidemiology; Immunity; Malaria; Meta-analysis; Plasmodium falciparum; Pregnancy; Systematic review.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
Publication types
MeSH terms
Grants and funding
- 1166753/National Health and Medical Research Council (AU)/International
- 1104975/National Health and Medical Research Council/International
- 1134989/Australian Centre of Research Excellence in Malaria Elimination (ACREME)/International
- 1134989/Australian Centre of Research Excellence in Malaria Elimination (ACREME)/International
- FT130101122/Australian Research Council/International
LinkOut - more resources
Full Text Sources
Miscellaneous
