

A pilot randomized controlled trial of 7 versus 14 days of antibiotic treatment for bloodstream infection on non-intensive care versus intensive care wards
- PMID: 31941546
- PMCID: PMC6964073
- DOI: 10.1186/s13063-019-4033-9
A pilot randomized controlled trial of 7 versus 14 days of antibiotic treatment for bloodstream infection on non-intensive care versus intensive care wards
Abstract
Background: The optimal treatment duration for patients with bloodstream infection is understudied. The Bacteremia Antibiotic Length Actually Needed for Clinical Effectiveness (BALANCE) pilot randomized clinical trial (RCT) determined that it was feasible to enroll and randomize intensive care unit (ICU) patients with bloodstream infection to 7 versus 14 days of treatment, and served as the vanguard for the ongoing BALANCE main RCT. We performed this BALANCE-Ward pilot RCT to examine the feasibility and impact of potentially extending the BALANCE main RCT to include patients hospitalized on non-ICU wards.
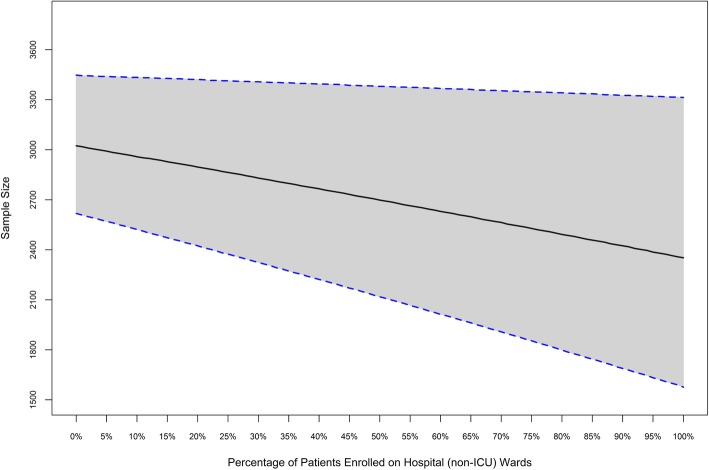
Methods: We conducted an open pilot RCT among a subset of six sites participating in the ongoing BALANCE RCT, randomizing patients with positive non-Staphylococcus aureus blood cultures on non-ICU wards to 7 versus 14 days of antibiotic treatment. The co-primary feasibility outcomes were recruitment rate and adherence to treatment duration protocol. We compared feasibility outcomes, patient/pathogen characteristics, and overall outcomes among those enrolled in this BALANCE-Ward and prior BALANCE-ICU pilot RCTs. We estimated the sample size and non-inferiority margin impacts of expanding the BALANCE main RCT to include non-ICU patients.
Results: A total of 134 patients were recruited over 47 site-months (mean 2.9 patients/site-month, median 1.0, range 0.1-4.4 patients/site-month). The overall recruitment rate exceeded the BALANCE-ICU pilot RCT (mean 1.10 patients/site-month, p < 0.0001). Overall protocol adherence also exceeded the adherence in the BALANCE-ICU pilot RCT (125/134, 93% vs 89/115, 77%, p = 0.0003). BALANCE-Ward patients were older, with lower Sequential Organ Failure Assessment scores, and higher proportions of infections caused by Escherichia coli and genito-urinary sources of bloodstream infection. The BALANCE-Ward pilot RCT patients had an overall 90-day mortality rate of 17/133 (12.8%), which was comparable to the 90-day mortality rate in the ICU pilot RCT (17/115, 14.8%) (p = 0.65). Simulation models indicated there would be minimal sample size and non-inferiority margin implications of expanding enrolment to increasing proportions of non-ICU versus ICU patients.
Conclusion: It is feasible to enroll non-ICU patients in a trial of 7 versus 14 days of antibiotics for bloodstream infection, and expanding the BALANCE RCT hospital-wide has the potential to improve the timeliness and generalizability of trial results.
Trial registration: Clinicaltrials.gov, NCT02917551. Registered on September 28, 2016.
Keywords: Bacteremia; Bloodstream infection; Critical care; Duration of treatment; Intensive care.
Conflict of interest statement
Dr. Rob Fowler is supported by a personnel award from the Heart and Stroke Foundation, Ontario Provincial Office. Dr. Deborah Cook holds a Canada Research Chair of Research Transfer in Intensive Care.
Figures



References
-
- World Health Organization Antimicrobial Resistance. Global Report on Surveillance 2014: WHO; 2014. https://www.who.int/drugresistance/documents/surveillancereport/en/.
-
- Harris PNA, Tambyah PA, Lye DC, et al. Effect of piperacillin-tazobactam vs meropenem on 30-day mortality for patients with E. coli or Klebsiella pneumoniae bloodstream infection and ceftriaxone resistance: A randomized clinical trial. JAMA. 2018;320(10):984–994. doi: 10.1001/jama.2018.12163. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
