

Major cardiac events for adult survivors of childhood cancer diagnosed between 1970 and 1999: report from the Childhood Cancer Survivor Study cohort
- PMID: 31941657
- PMCID: PMC7190022
- DOI: 10.1136/bmj.l6794
Major cardiac events for adult survivors of childhood cancer diagnosed between 1970 and 1999: report from the Childhood Cancer Survivor Study cohort
Abstract
Objective: To investigate the impact of modifications to contemporary cancer protocols, which minimize exposures to cardiotoxic treatments and preserve long term health, on serious cardiac outcomes among adult survivors of childhood cancer.
Design: Retrospective cohort study.
Setting: 27 institutions participating in the Childhood Cancer Survivor Study.
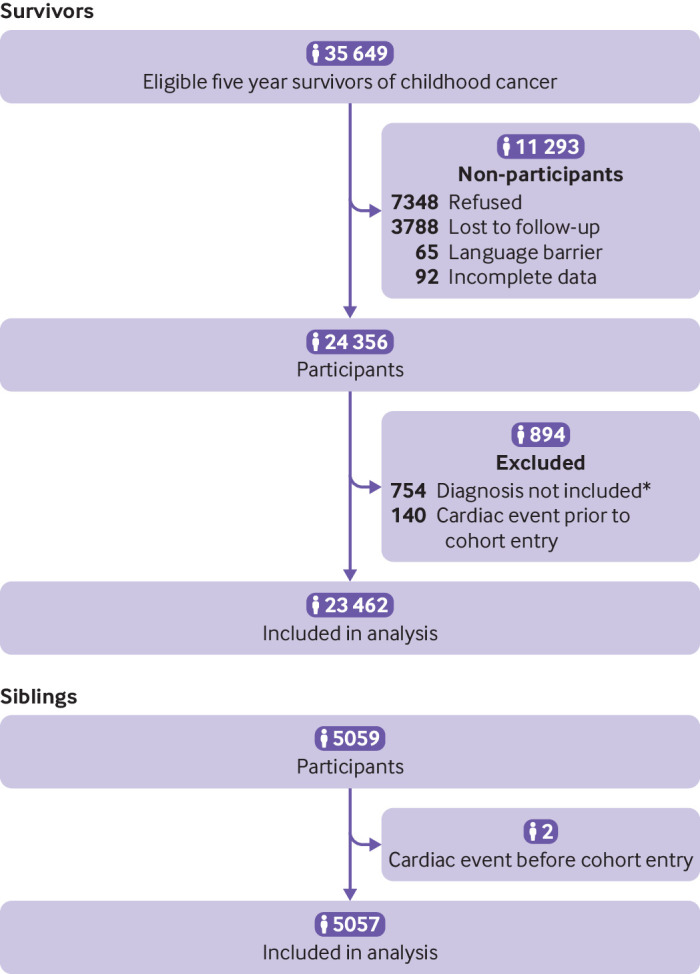
Participants: 23 462 five year survivors (6193 (26.4%) treated in the 1970s, 9363 (39.9%) treated in the 1980s, and 7906 (33.6%) treated in the 1990s) of leukemia, brain cancer, Hodgkin lymphoma, non-Hodgkin lymphoma, renal tumors, neuroblastoma, soft tissue sarcomas, and bone sarcomas diagnosed prior to age 21 years between 1 January 1970 and 31 December 1999. Median age at diagnosis was 6.1 years (range 0-20.9) and 27.7 years (8.2-58.3) at last follow-up. A comparison group of 5057 siblings of cancer survivors were also included.
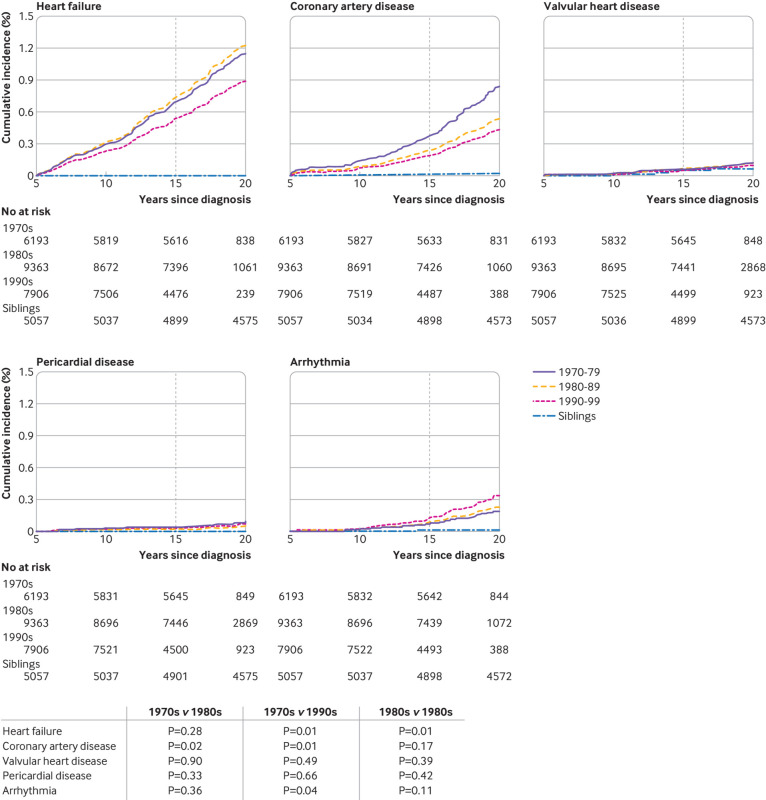
Main outcome measures: Cumulative incidence and 95% confidence intervals of reported heart failure, coronary artery disease, valvular heart disease, pericardial disease, and arrhythmias by treatment decade. Events were graded according to the National Cancer Institute's Common Terminology Criteria for Adverse Events. Multivariable subdistribution hazard models were used to estimate hazard ratios by decade, and mediation analysis examined risks with and without exposure to cardiotoxic treatments.
Results: The 20 year cumulative incidence of heart failure (0.69% for those treated in the 1970s, 0.74% for those treated in the 1980s, 0.54% for those treated in the 1990s) and coronary artery disease (0.38%, 0.24%, 0.19%, respectively), decreased in more recent eras (P<0.01), though not for valvular disease (0.06%, 0.06%, 0.05%), pericardial disease (0.04%, 0.02%, 0.03%), or arrhythmias (0.08%, 0.09%, 0.13%). Compared with survivors with a diagnosis in the 1970s, the risk of heart failure, coronary artery disease, and valvular heart disease decreased in the 1980s and 1990s but only significantly for coronary artery disease (hazard ratio 0.65, 95% confidence interval 0.45 to 0.92 and 0.53, 0.36 to 0.77, respectively). The overall risk of coronary artery disease was attenuated by adjustment for cardiac radiation (0.90, 0.78 to 1.05), particularly among survivors of Hodgkin lymphoma (unadjusted for radiation: 0.77, 0.66 to 0.89; adjusted for radiation: 0.87, 0.69 to 1.10).
Conclusions: Historical reductions in exposure to cardiac radiation have been associated with a reduced risk of coronary artery disease among adult survivors of childhood cancer. Additional follow-up is needed to investigate risk reductions for other cardiac outcomes.
Trial registration: ClinicalTrials.gov NCT01120353.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare support from the National Cancer Institute (CA55727, to GTA, principal investigator) for the Childhood Cancer Survivor Study; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
Falling risk of heart disease among survivors of childhood cancer.BMJ. 2020 Jan 15;368:m58. doi: 10.1136/bmj.m58. BMJ. 2020. PMID: 31941703 No abstract available.
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical