

Supraventricular tachycardia: An overview of diagnosis and management
- PMID: 31941731
- PMCID: PMC6964177
- DOI: 10.7861/clinmed.cme.20.1.3
Supraventricular tachycardia: An overview of diagnosis and management
Abstract
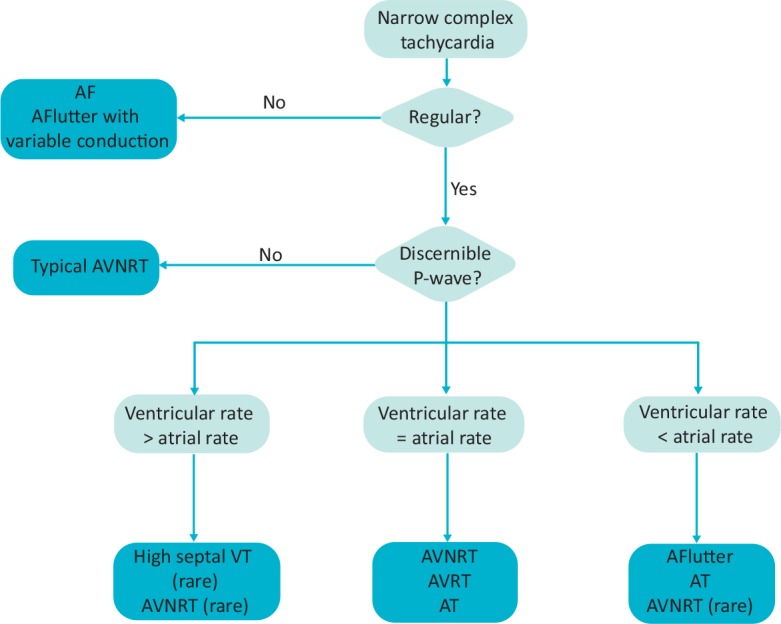
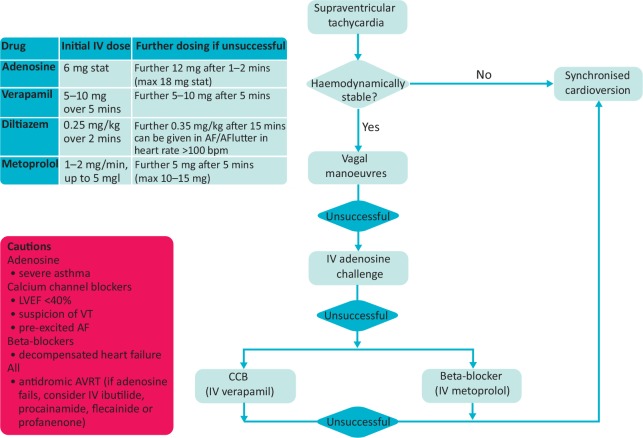
Supraventricular tachycardia (SVT) is a common cause of hospital admissions and can cause significant patient discomfort and distress. The most common SVTs include atrioventricular nodal re-entrant tachycardia, atrioventricular re-entrant tachycardia and atrial tachycardia. In many cases, the underlying mechanism can be deduced from electrocardiography during tachycardia, comparing it with sinus rhythm, and assessing the onset and offset of tachycardia. Recent European Society of Cardiology guidelines continue to advocate the use of vagal manoeuvres and adenosine as first-line therapies in the acute diagnosis and management of SVT. Alternative therapies include the use of beta-blockers and calcium channel blockers. All patients treated for SVT should be referred for a heart rhythm specialist opinion. Long-term treatment is dependent on several factors including frequency of symptoms, risk stratification, and patient preference. Management can range from conservative, if symptoms are rare and the patient is low risk, to catheter ablation which is curative in the majority of patients.
Keywords: ECG; SVT; Supraventricular tachycardia; arrhythmia; narrow complex tachycardia.
© Royal College of Physicians 2020. All rights reserved.
Figures
References
-
- Katritsis DG, Boriani G, Cosio FG, et al. European Heart Rhythm Association (EHRA) consensus document on the management of supraventricular arrhythmias, endorsed by Heart Rhythm Society (HRS), Asia-Pacific Heart Rhythm Society (APHRS), and Sociedad Latinoamericana de Estimulación Cardiaca y Elect. Eur Heart J 2018;39:1442–5. - PubMed
-
- Brugada J, Katritsis DG, Arbelo E, et al. 2019 ESC guidelines for the management of patients with supraventricular tachycardia. The Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC). Eur Heart J 2019:ehz467. - PubMed
-
- Lee KW, Badhwar N, Scheinman MM. Supraventricular tachycardia – part I. Curr Probl Cardiol 2008;33:467–546. - PubMed
-
- Kalbfleisch SJ, El-Atassi R, Calkins H, Langberg JJ, Morady F. Differentiation of paroxysmal narrow QRS complex tachycardias using the 12-lead electrocardiogram. J Am Coll Cardiol 1993;21:85–9. - PubMed
-
- Orejarena LA, Vidaillet H, Destefano F, et al. Paroxysmal supraventricular tachycardia in the general population. J Am Coll Cardiol 1998;31:150–7. - PubMed
