

Benefits of re-do surgery for recurrent intracranial meningiomas
- PMID: 31941981
- PMCID: PMC6962359
- DOI: 10.1038/s41598-019-57254-5
Benefits of re-do surgery for recurrent intracranial meningiomas
Abstract
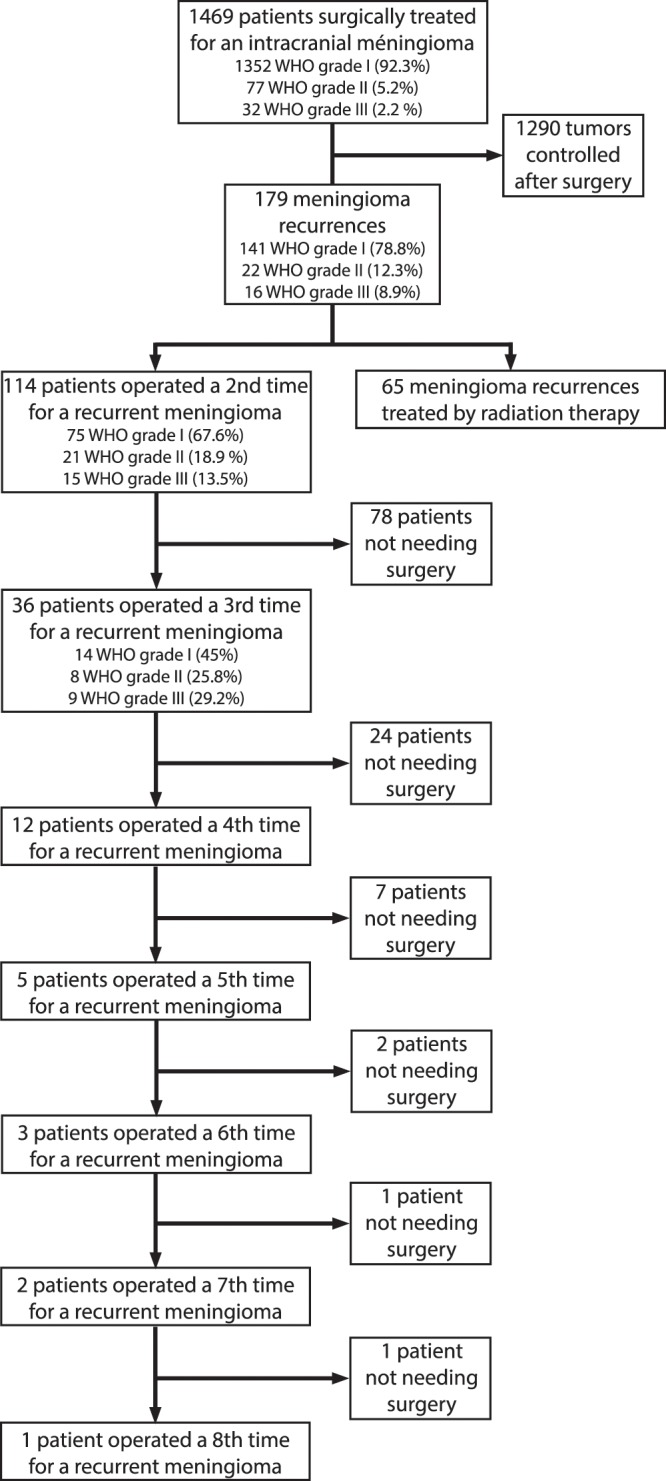
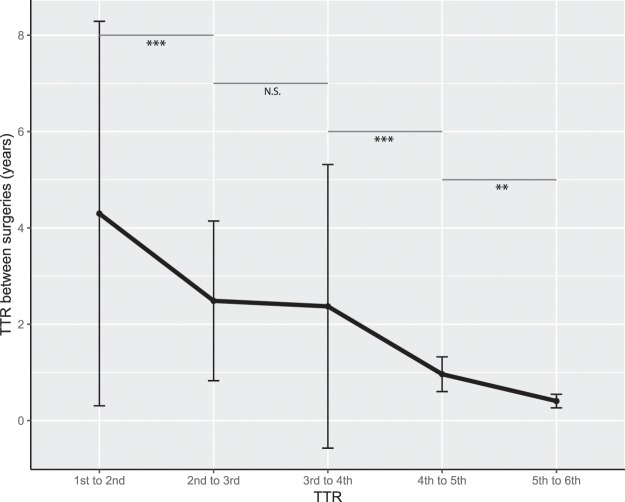
Meningiomas are the most common intracranial extra-axial tumor. While the literature is abundant on the therapeutic management of meningioma recurrence after the initial surgery, the natural history of repeated recurrences is poorly described, as well as and their respective management. A partly retrospective, partly prospective review was conducted in a Norwegian cohort of 1469 consecutive cases of meningioma surgically treated, totaling 11 414 patient-years of follow-up. 114 recurrences (7.7%) were treated surgically with a risk a surgical retreatment of 1% per patient-year of follow-up. 36 patients were operated on 3 times or more. The time-to-retreatment (TTR) decreased significantly and steadily between surgeries, from 4.3 ± 4 years after the first surgery to 2.4 ± 2.9 years after the third surgery. The primary driver for recurrence was the WHO grade (OR 7.13 [4.40;11.55], p < 0.001 for the first recurrence and OR 4.13 [1.49;12.15], p 0.008 for the second), the second predictive factor being a skull base location (OR 2.76 [1.95;3.99] p < 0.001 and OR 0.24 [0.09;0.65], p0.006 respectively). The rates of postoperative hematomas and infections were not influenced by the number of surgeries, whereas the rate of postoperative neurological worsening increased from 3.9% to 16.6% and 13.9%, respectively, after the first, second, and third surgeries. We observed that the TTR decreased significantly between surgeries in patients requiring repeated resections, indicating that surgical treatment of recurrences does not reset the clock but is indeed a "race against time". This should be considered when assessing the benefit-to-risk ratio of patients undergoing repeated surgeries for a recurrent meningioma.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
