

B cells and tertiary lymphoid structures promote immunotherapy response
- PMID: 31942075
- PMCID: PMC8762581
- DOI: 10.1038/s41586-019-1922-8
B cells and tertiary lymphoid structures promote immunotherapy response
Abstract
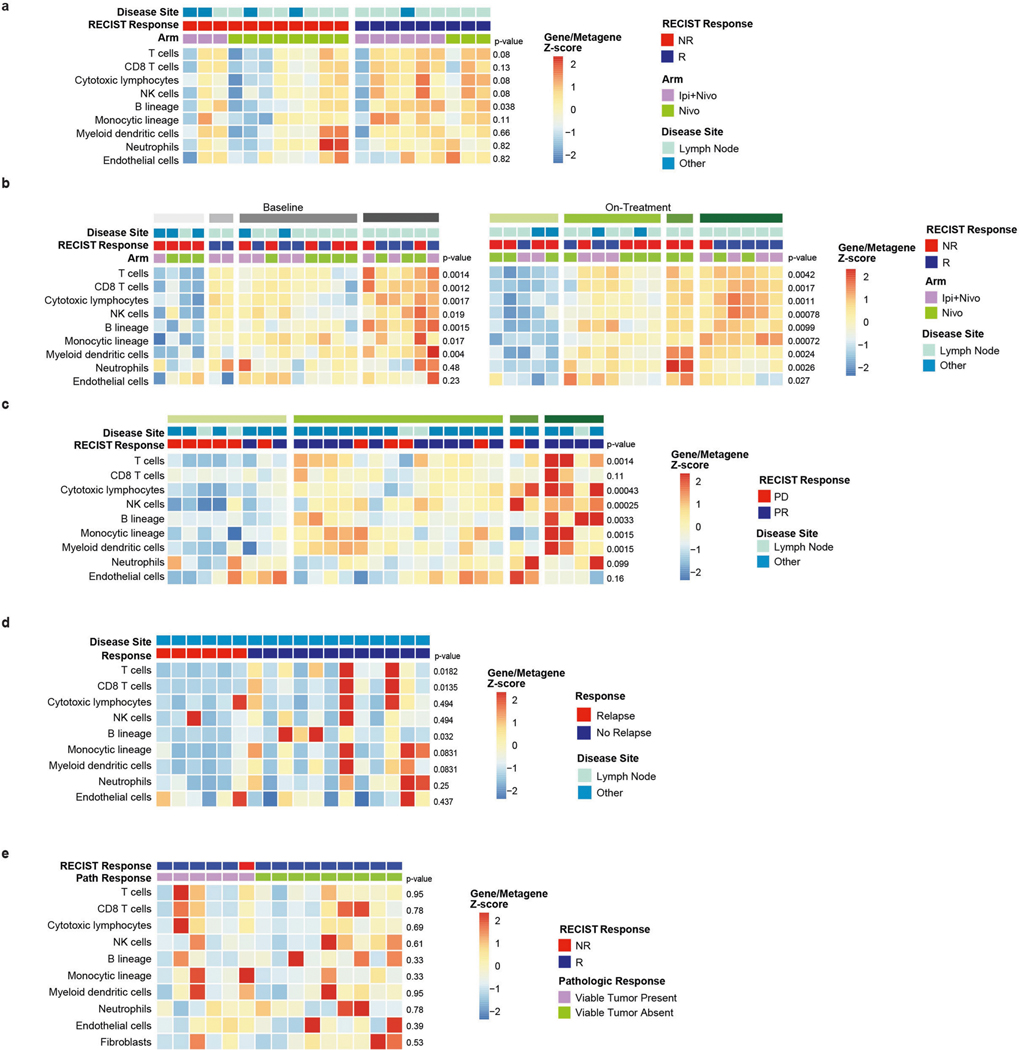
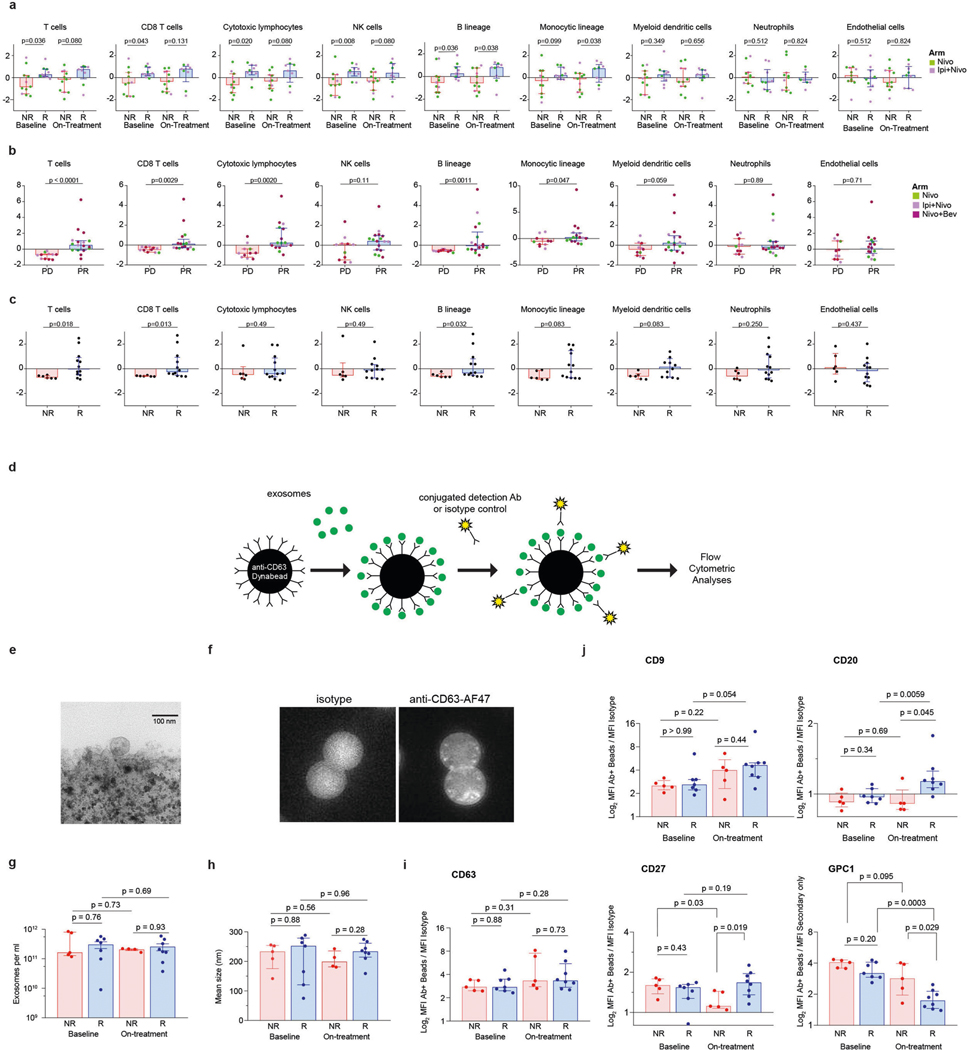
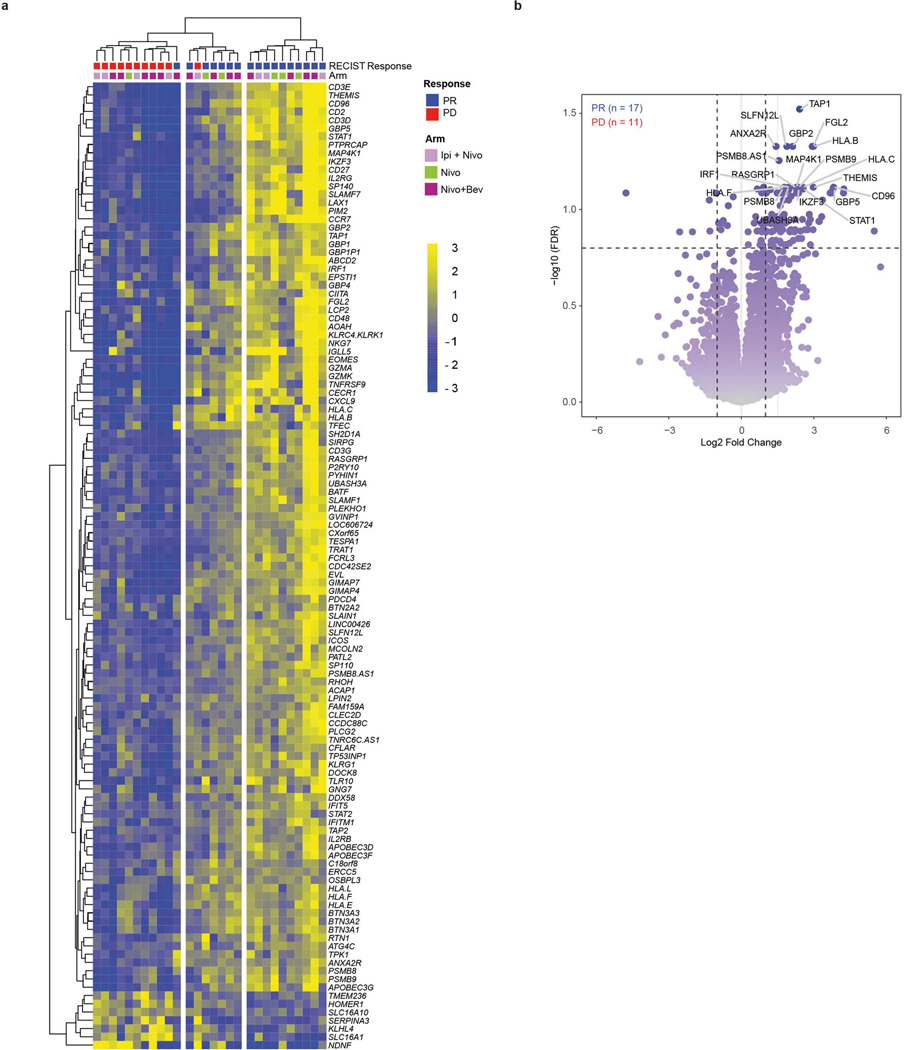
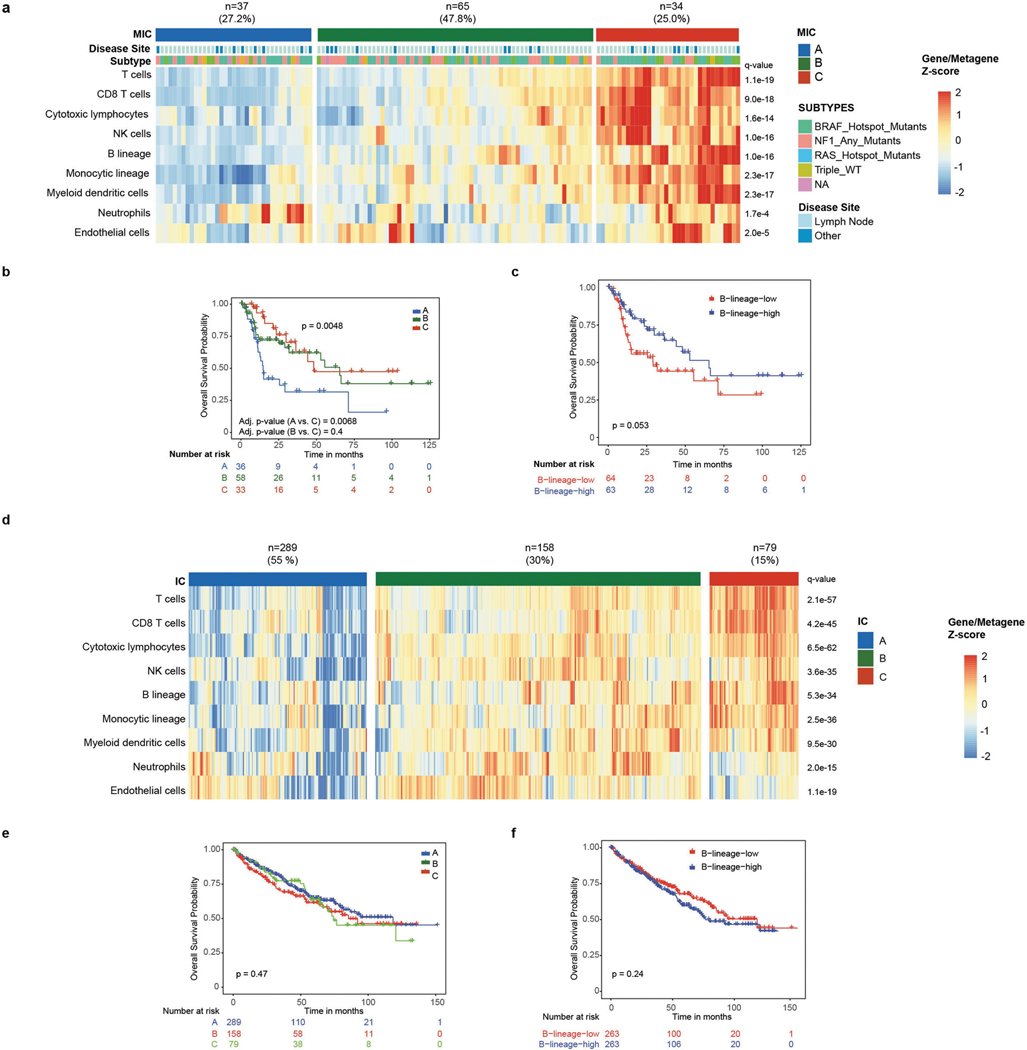
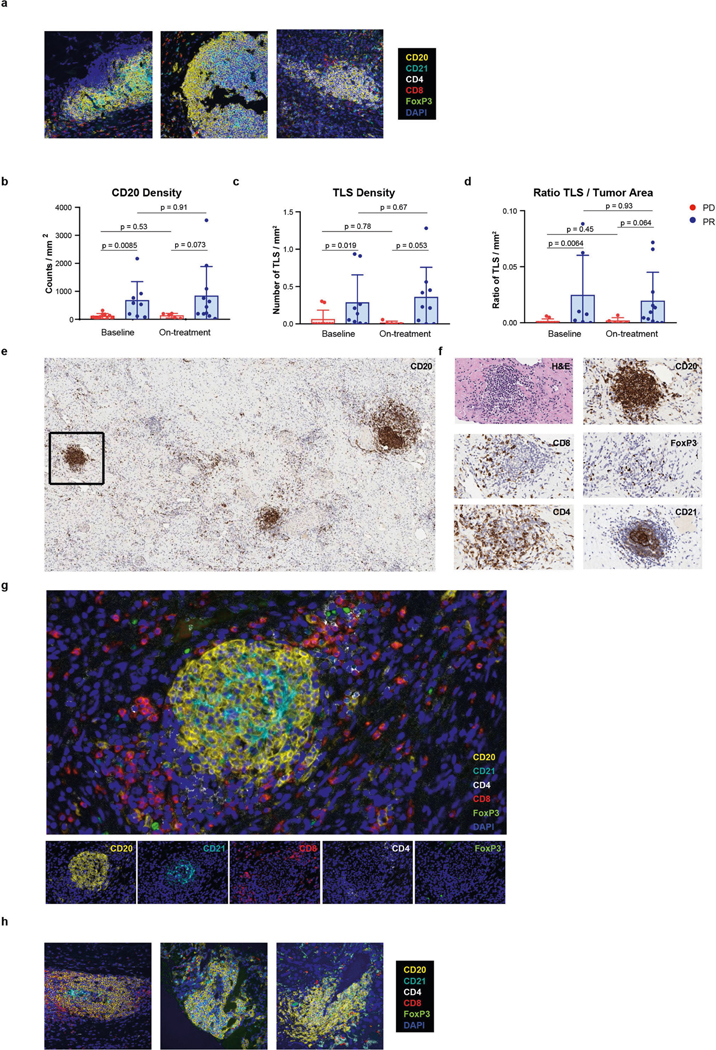
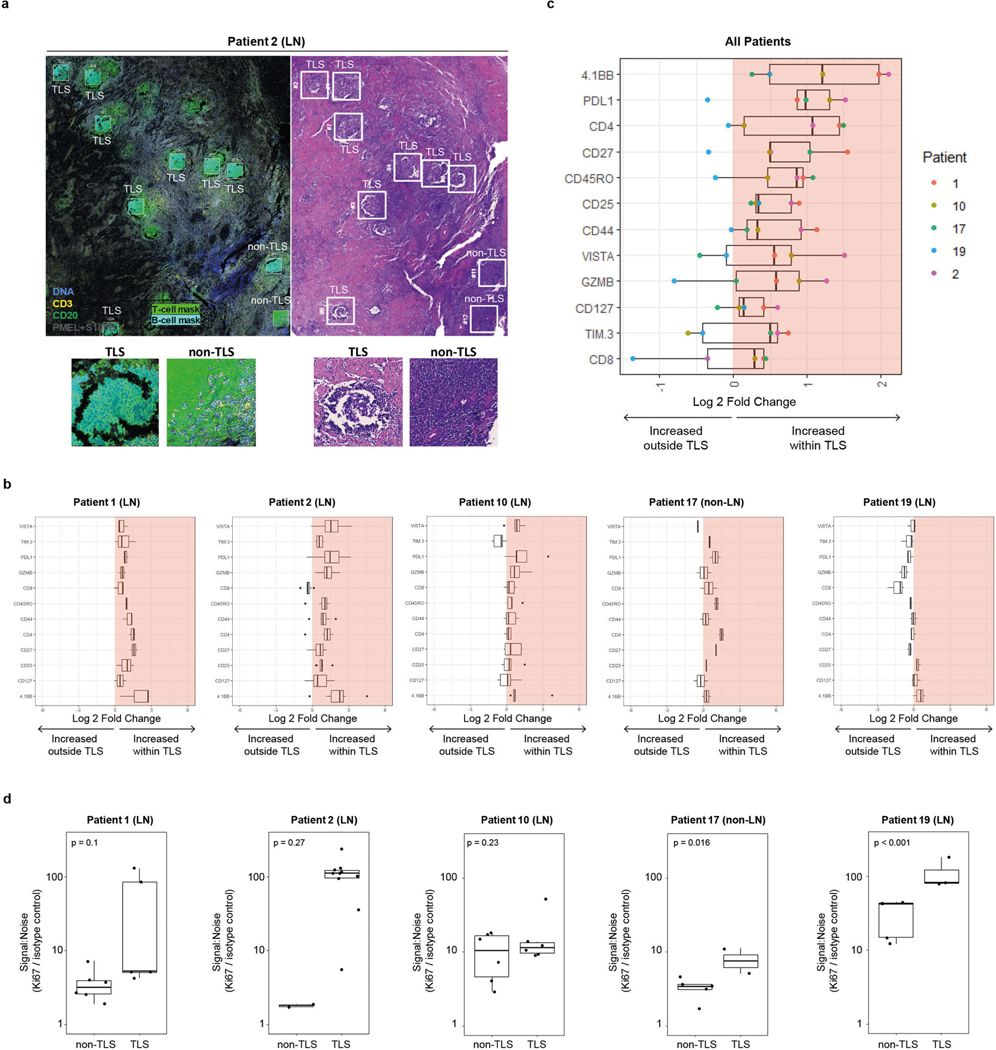
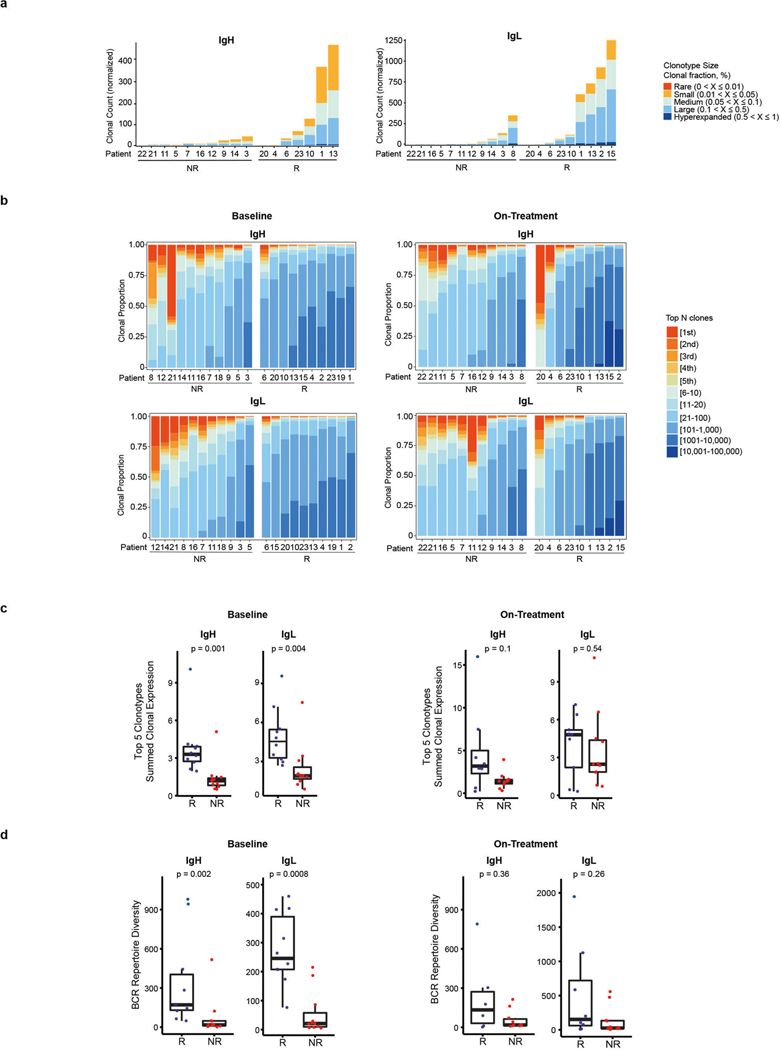
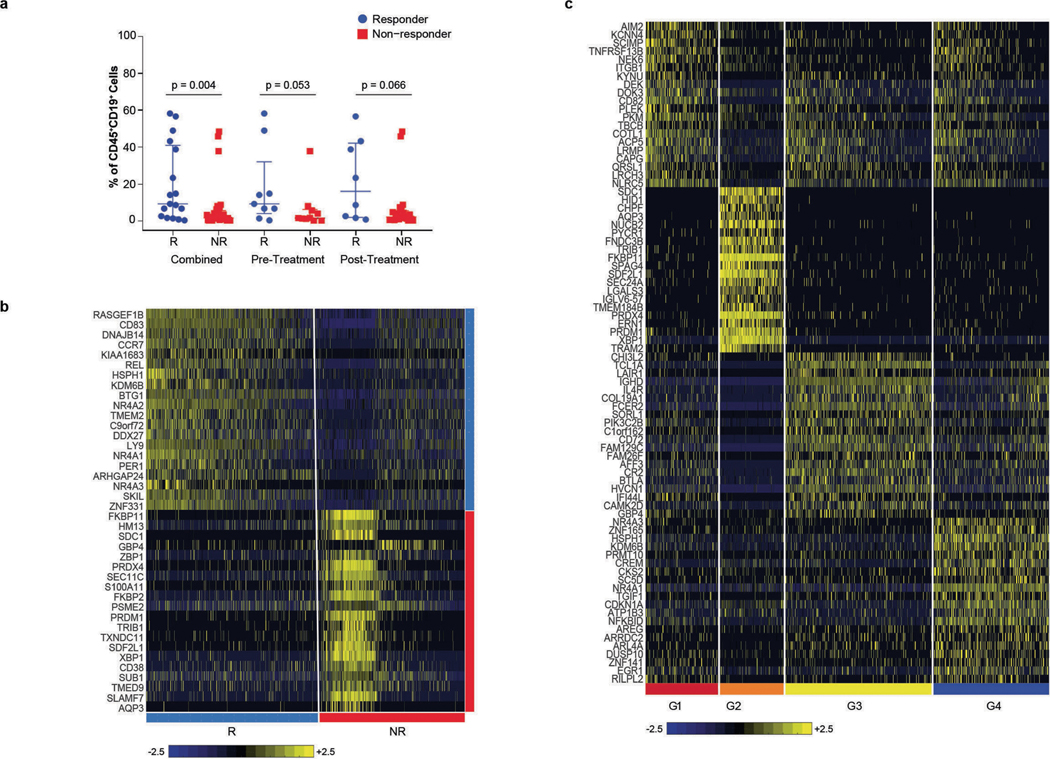
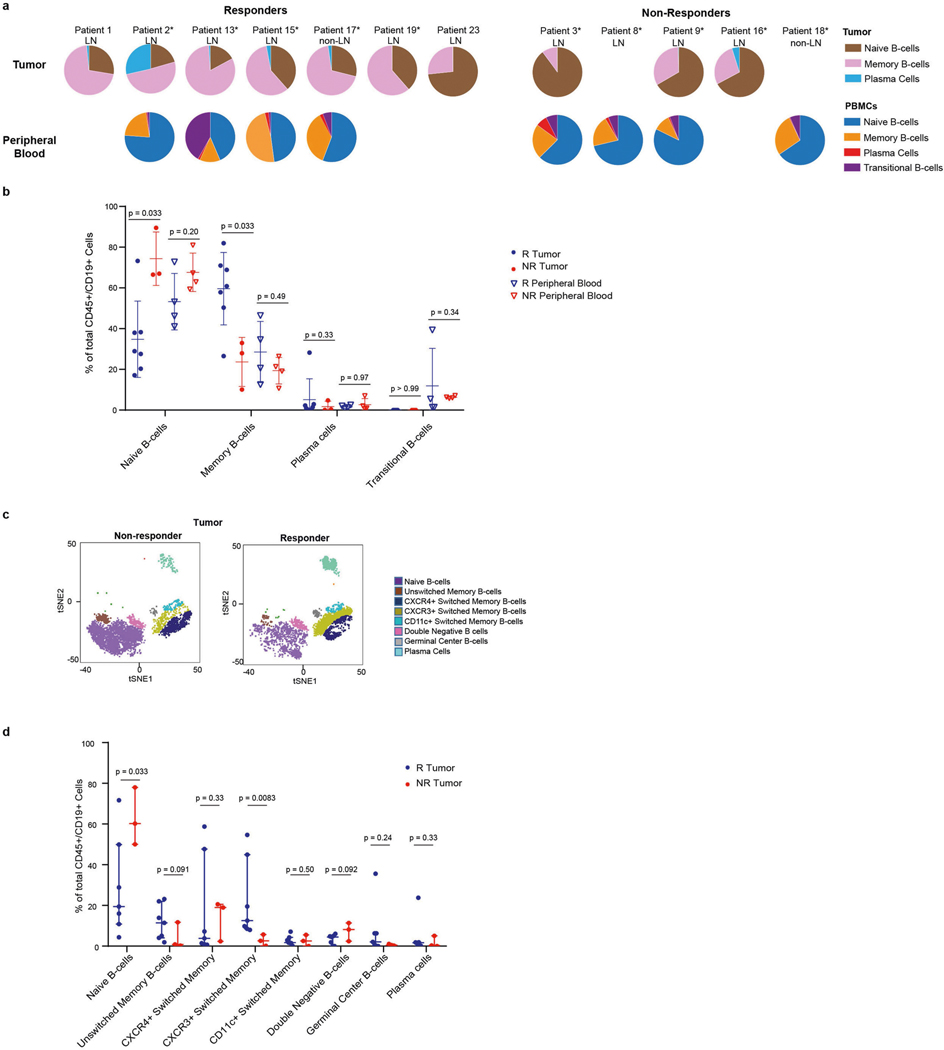
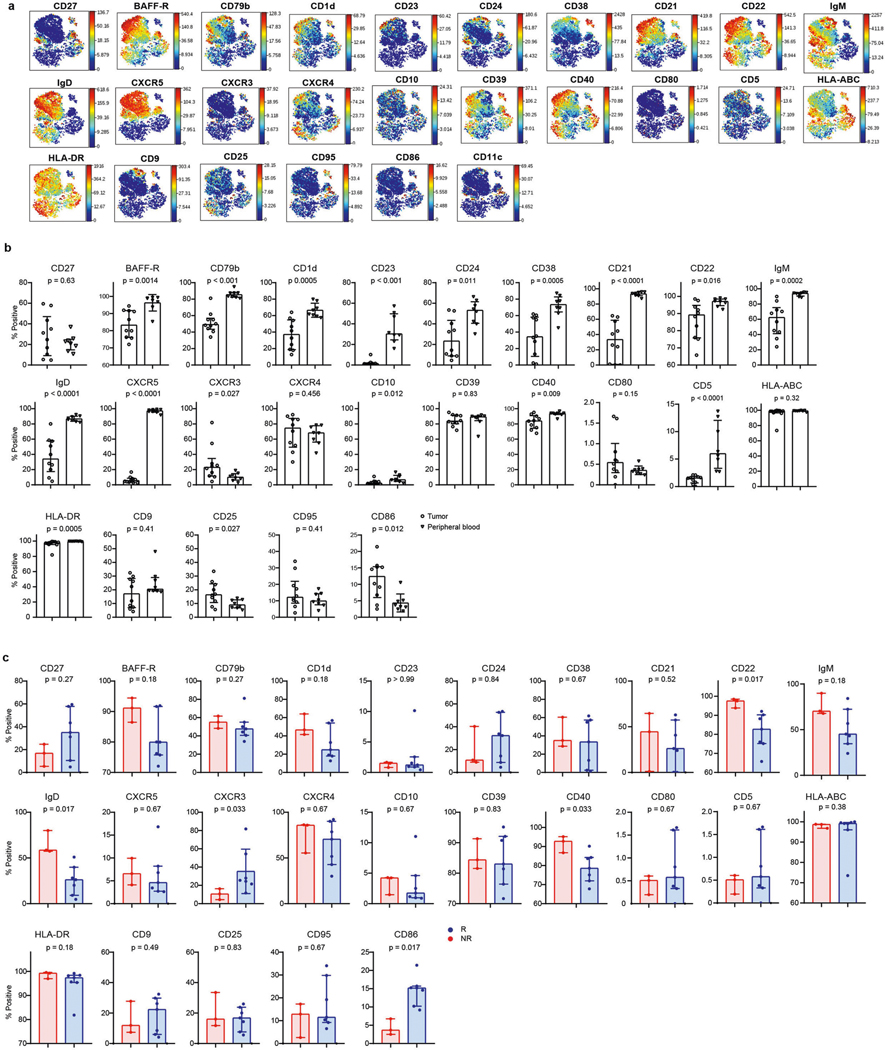
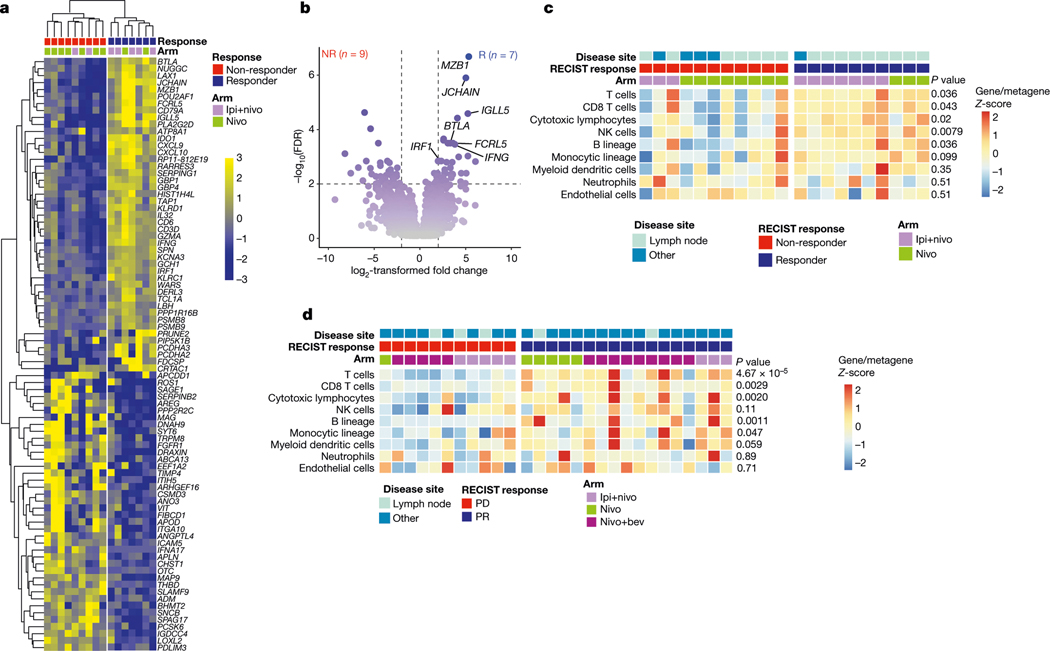
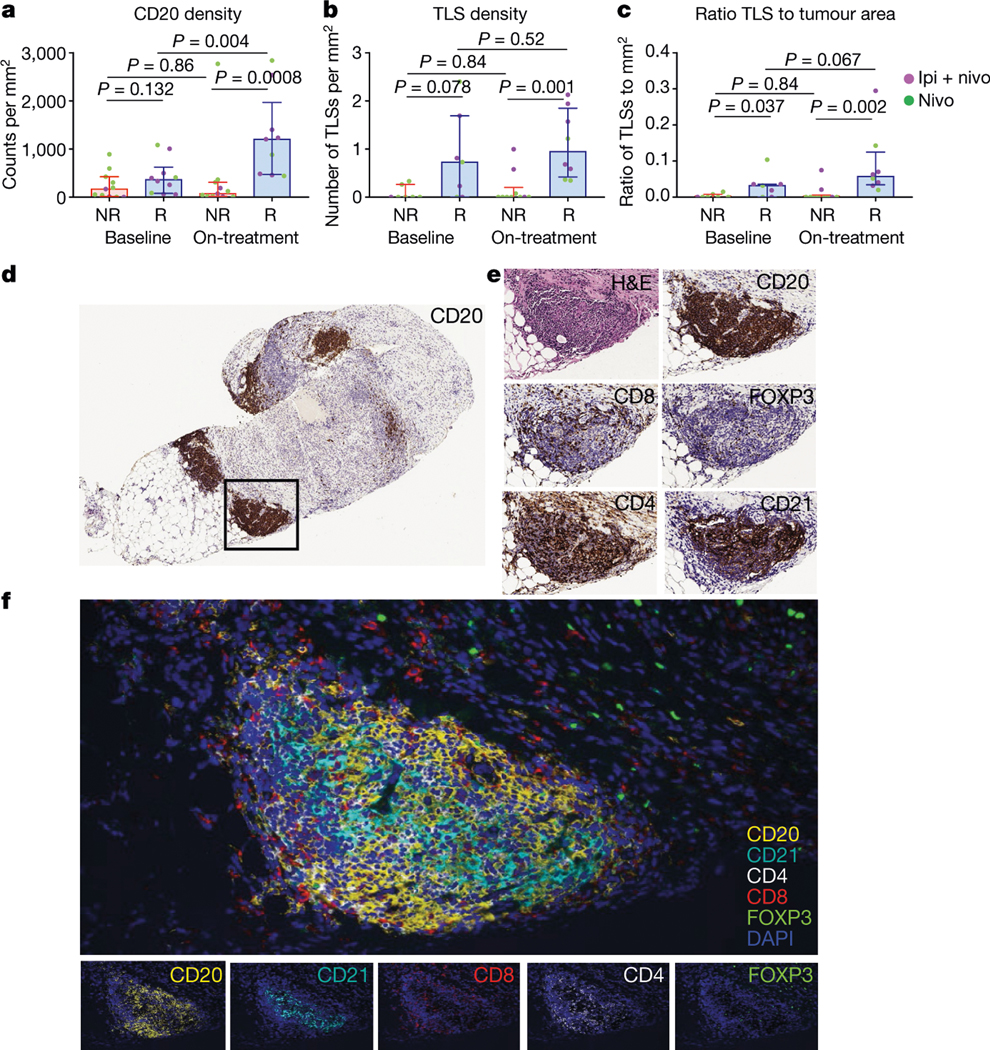
Treatment with immune checkpoint blockade (ICB) has revolutionized cancer therapy. Until now, predictive biomarkers1-10 and strategies to augment clinical response have largely focused on the T cell compartment. However, other immune subsets may also contribute to anti-tumour immunity11-15, although these have been less well-studied in ICB treatment16. A previously conducted neoadjuvant ICB trial in patients with melanoma showed via targeted expression profiling17 that B cell signatures were enriched in the tumours of patients who respond to treatment versus non-responding patients. To build on this, here we performed bulk RNA sequencing and found that B cell markers were the most differentially expressed genes in the tumours of responders versus non-responders. Our findings were corroborated using a computational method (MCP-counter18) to estimate the immune and stromal composition in this and two other ICB-treated cohorts (patients with melanoma and renal cell carcinoma). Histological evaluation highlighted the localization of B cells within tertiary lymphoid structures. We assessed the potential functional contributions of B cells via bulk and single-cell RNA sequencing, which demonstrate clonal expansion and unique functional states of B cells in responders. Mass cytometry showed that switched memory B cells were enriched in the tumours of responders. Together, these data provide insights into the potential role of B cells and tertiary lymphoid structures in the response to ICB treatment, with implications for the development of biomarkers and therapeutic targets.
Conflict of interest statement
Figures


Comment in
-
New predictors for immunotherapy responses sharpen our view of the tumour microenvironment.Nature. 2020 Jan;577(7791):474-476. doi: 10.1038/d41586-019-03943-0. Nature. 2020. PMID: 31965091 Free PMC article.
-
B cells and TLSs facilitate a response to ICI.Nat Rev Clin Oncol. 2020 Apr;17(4):195. doi: 10.1038/s41571-020-0338-6. Nat Rev Clin Oncol. 2020. PMID: 32024979 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
