

Association of Prediabetes With CKD Progression and Adverse Cardiovascular Outcomes: An Analysis of the CRIC Study
- PMID: 31943096
- PMCID: PMC7069215
- DOI: 10.1210/clinem/dgaa017
Association of Prediabetes With CKD Progression and Adverse Cardiovascular Outcomes: An Analysis of the CRIC Study
Abstract
Purpose: Despite our understanding of diabetes as an established risk factor for progressive kidney disease and cardiac complications, the prognostic significance of prediabetes in patients with chronic kidney disease (CKD) remains largely unknown.
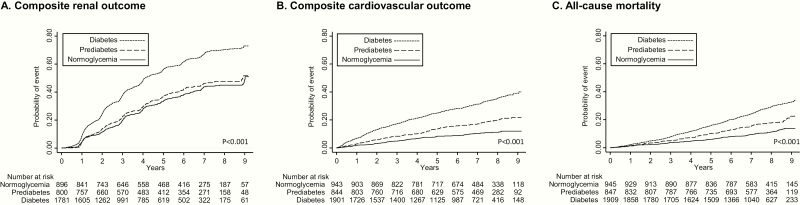
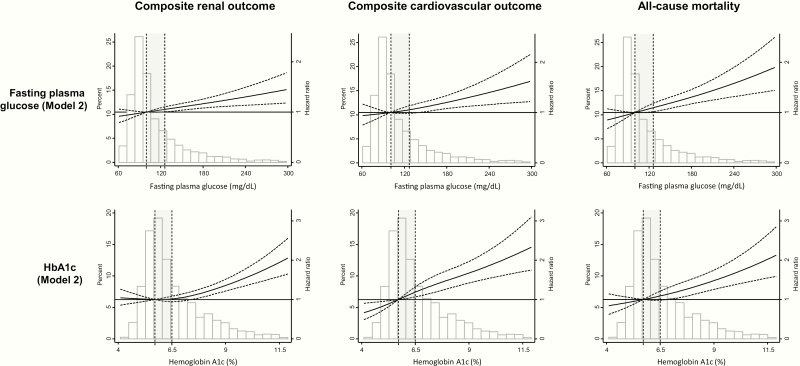
Methods: Participants of the Chronic Renal Insufficiency Cohort (CRIC) were categorized as having normoglycemia, prediabetes, or diabetes according to fasting plasma glucose, glycated hemoglobin A1c (HbA1c), and treatment with antidiabetic drugs at baseline. Unadjusted and adjusted proportional hazards models were fit to estimate the association of prediabetes and diabetes (versus normoglycemia) with: (1) composite renal outcome (end-stage renal disease, 50% decline in estimated glomerular filtration rate to ≤ 15 mL/min/1.73 m2, or doubling of urine protein-to-creatinine ratio to ≥ 0.22 g/g creatinine); (2) composite cardiovascular (CV) outcome (congestive heart failure, myocardial infarction or stroke); and (3) all-cause mortality.
Results: Of the 3701 individuals analyzed, 945 were normoglycemic, 847 had prediabetes and 1909 had diabetes. The median follow-up was 7.5 years. Prediabetes was not associated with the composite renal outcome (adjusted hazard ratio [aHR] 1.13; 95% confidence interval [CI], 0.96-1.32; P = 0.14), but was associated with proteinuria progression (aHR 1.23; 95% CI, 1.03-1.47; P = 0.02). Prediabetes was associated with a higher risk of the composite CV outcome (aHR 1.38; 95% CI, 1.05-1.82; P = 0.02) and a trend towards all-cause mortality (aHR 1.28; 95% CI, 0.99-1.66; P = 0.07). Participants with diabetes had an increased risk of the composite renal outcome, the composite CV outcome, and all-cause mortality.
Conclusions: In individuals with CKD, prediabetes was not associated with composite renal outcome, but was associated with an increased risk of proteinuria progression and adverse CV outcomes.
Keywords: all-cause mortality; cardiovascular outcomes; chronic kidney disease; diabetes; prediabetes; renal outcomes.
© Endocrine Society 2020. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Comment in
-
A Nuanced Relationship Between Prediabetes and Chronic Kidney Disease.J Clin Endocrinol Metab. 2020 Apr 1;105(4):dgaa079. doi: 10.1210/clinem/dgaa079. J Clin Endocrinol Metab. 2020. PMID: 32086934 No abstract available.
References
-
- CDC. National Diabetes Statistics Report, 2017. Atlanta, GA: Centers for Disease Control and Prevention; 2017.
-
- Gerstein HC, Santaguida P, Raina P, et al. Annual incidence and relative risk of diabetes in people with various categories of dysglycemia: a systematic overview and meta-analysis of prospective studies. Diabetes Res Clin Pract. 2007;78(3):305–312. - PubMed
-
- Eknoyan G, Lameire N, Eckardt K, et al. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. 2013;3(1):5–14. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
