

Efficacy and safety of sodium zirconium cyclosilicate for hyperkalaemia: the randomized, placebo-controlled HARMONIZE-Global study
- PMID: 31944628
- PMCID: PMC7083449
- DOI: 10.1002/ehf2.12561
Efficacy and safety of sodium zirconium cyclosilicate for hyperkalaemia: the randomized, placebo-controlled HARMONIZE-Global study
Abstract
Aims: Sodium zirconium cyclosilicate (SZC, formerly ZS-9) is a selective K+ binder to treat adults with hyperkalaemia. HARMONIZE-Global examined the efficacy and safety of SZC among outpatients with hyperkalaemia from diverse geographic and ethnic origins.
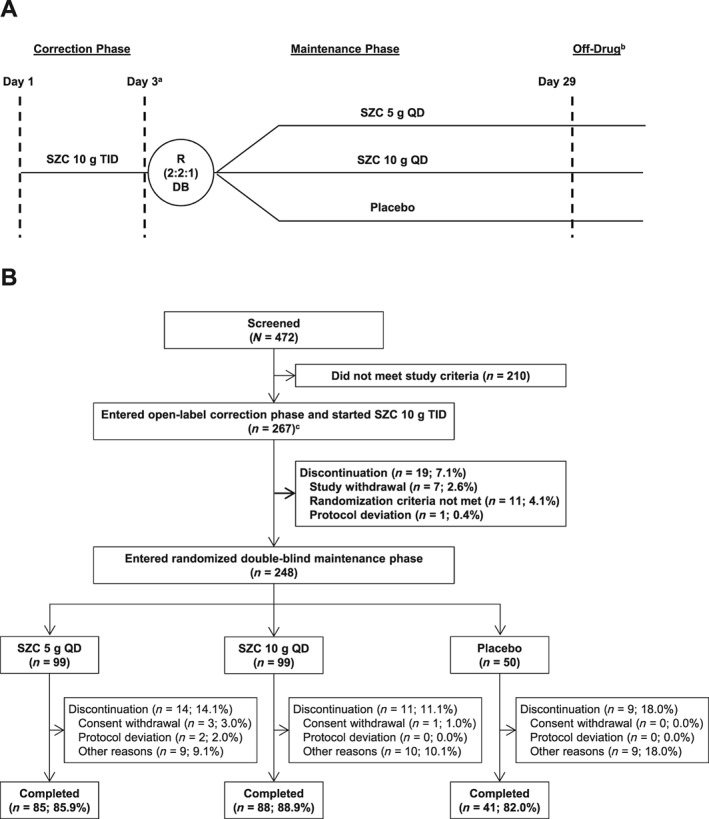
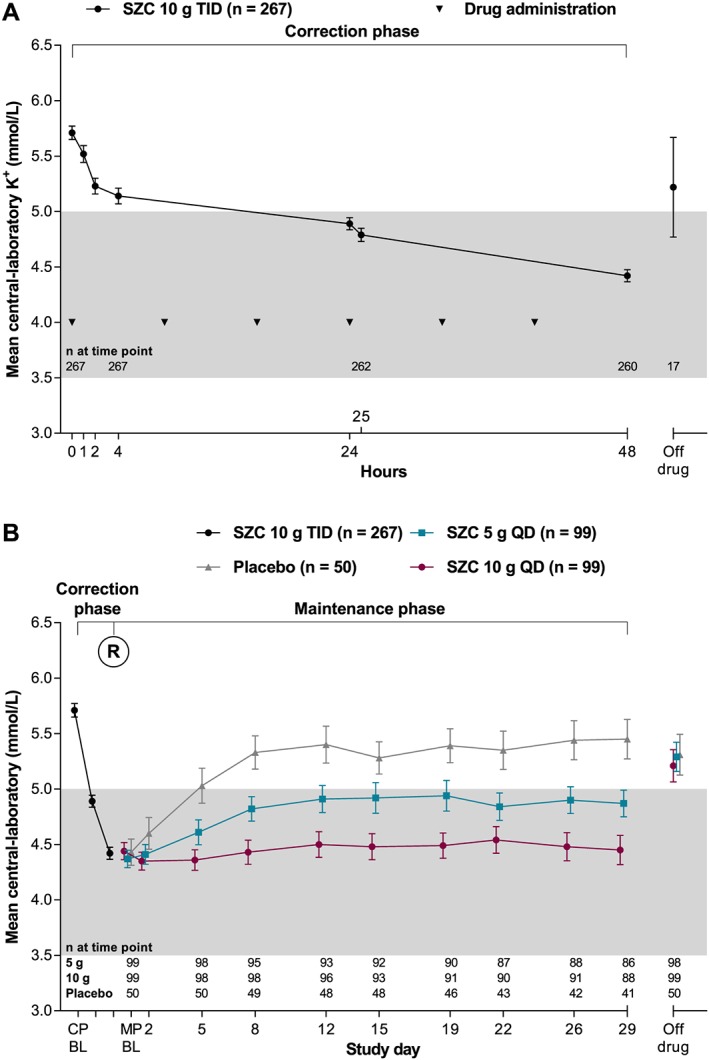
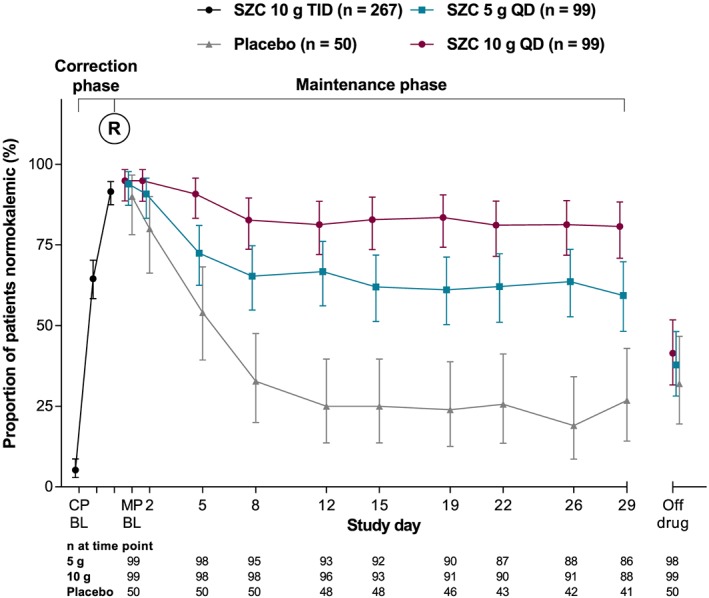
Methods and results: This phase 3, randomized, double-blind, placebo-controlled study recruited outpatients with serum K+ ≥5.1 mmol/L (measured by point-of-care i-STAT device) at 45 sites in Japan, Russia, South Korea, and Taiwan. Following open-label treatment with thrice-daily SZC 10 g during a 48 h correction phase (CP), patients achieving normokalaemia (K+ 3.5-5.0 mmol/L) were randomized 2:2:1 to once-daily SZC 5 g, SZC 10 g, or placebo during a 28 day maintenance phase (MP). The primary endpoint was mean central-laboratory K+ level during days 8-29 of the MP. Of 267 patients in the CP, 248 (92.9%) entered the MP. During the CP, mean central-laboratory K+ was reduced by 1.28 mmol/L at 48 h vs. baseline (P < 0.001). During the MP (days 8-29), SZC 5 and 10 g once-daily significantly lowered mean central-laboratory K+ by 9.6% and 17.7%, respectively, vs. placebo (P < 0.001 for both). More patients had normokalaemia (central-laboratory K+ 3.5-5.0 mmol/L at day 29) with SZC 5 (58.6%) and 10 g (77.3%) vs. placebo (24.0%), with the greatest number of normokalaemic days in the 10-g group. The most common adverse events with SZC were mild or moderate constipation and oedema.
Conclusions: Normokalaemia achieved during the CP was maintained over 28 days with SZC treatment among outpatients with hyperkalaemia.
Keywords: Hyperkalaemia; Normokalaemia; Potassium; Sodium zirconium cyclosilicate.
© 2020 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology.
Conflict of interest statement
F.Z. reports consultancy, steering committee, and/or speaker fees from Amgen, AstraZeneca, Bayer, Boehringer, Boston Scientific, Cardior, CVRx, General Electric Healthcare, Janssen, Novartis, Quantum Genomics, Resmed, and Vifor‐Fresenius and also reports being founder of CardioRenal. B.G.H., Y.M., S.K.S., and E.M.V. declared no conflict of interest. M.R., S.E., and J.Z. are full‐time employees of AstraZeneca.
Figures
References
-
- Rossignol P, Legrand M, Kosiborod M, Hollenberg SM, Peacock WF, Emmett M, Epstein M, Kovesdy CP, Yilmaz MB, Stough WG, Gayat E, Pitt B, Zannad F, Mebazaa A. Emergency management of severe hyperkalemia: guideline for best practice and opportunities for the future. Pharmacol Res 2016; 113: 585–591. - PubMed
-
- Di Lullo L, Ronco C, Granata A, Paoletti E, Barbera V, Cozzolino M, Ravera M, Fusaro M, Bellasi A. Chronic hyperkalemia in cardiorenal patients: risk factors, diagnosis, and new treatment options. Cardiorenal Med 2019; 9: 8–21. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
