

Microbiome signatures in neonatal central line associated bloodstream infections
- PMID: 31945114
- PMCID: PMC6964844
- DOI: 10.1371/journal.pone.0227967
Microbiome signatures in neonatal central line associated bloodstream infections
Abstract
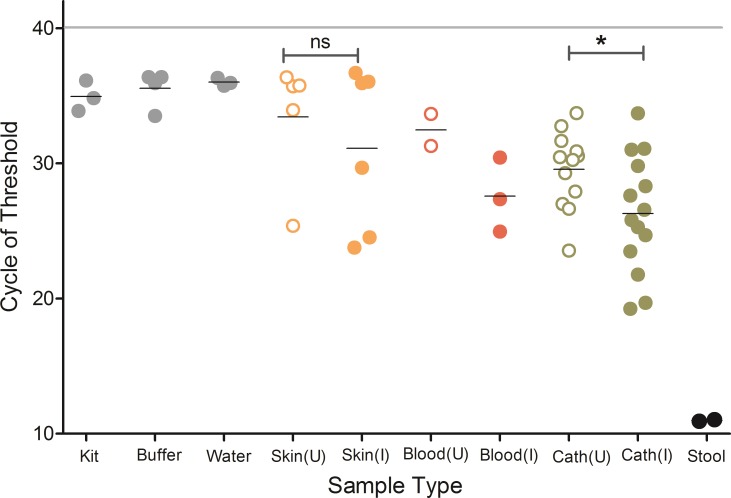
Neonates are at high risk for central line associated bloodstream infections (CLABSI). Biofilm formation is universal on indwelling catheters but why some biofilms seed the bloodstream to cause CLABSI is not clearly understood. With the objective to test the hypothesis that catheter biofilm microbiome in neonates with CLABSI differs than those without infection, we prospectively enrolled neonates (n = 30) with infected and uninfected indwelling central catheters. Catheters were collected at the time of removal, along with blood samples and skin swabs at the catheter insertion sites. Microbiomes of catheter biofilms, skin swabs and blood were evaluated by profiling the V4 region of the bacterial 16S rRNA gene using Illumina MiSeq sequencing platform. The microbial DNA load was higher from catheter biofilms of CLABSI patients without differences in alpha diversity when compared to that of the non-CLABSI neonates. Proteus and unclassified Staphylococcaceae were more abundant in infected catheter biofilms while Bradyrhizobium, Cloacibacterium, and Sphingomonas were more abundant in the uninfected catheters. A blood microbiome was detected in uninfected samples. The blood microbiome in CLABSI neonates clustered separately from the uninfected blood samples in beta diversity plots. We found that the microbiome signature in catheter biofilm and blood of neonates with CLABSI is different than the microbiomes of non-CLABSI neonates.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures




Similar articles
-
Biofilm microbiome in extracorporeal membrane oxygenator catheters.PLoS One. 2021 Sep 16;16(9):e0257449. doi: 10.1371/journal.pone.0257449. eCollection 2021. PLoS One. 2021. PMID: 34529734 Free PMC article.
-
Biofilm-based central line-associated bloodstream infections.Adv Exp Med Biol. 2015;830:157-79. doi: 10.1007/978-3-319-11038-7_10. Adv Exp Med Biol. 2015. PMID: 25366227 Review.
-
Risk of morbidity following catheter removal among neonates with catheter associated bloodstream infection.J Neonatal Perinatal Med. 2017;10(3):291-299. doi: 10.3233/NPM-16137. J Neonatal Perinatal Med. 2017. PMID: 28854516
-
Dwell time and risk of central-line-associated bloodstream infection in neonates.J Hosp Infect. 2017 Nov;97(3):267-274. doi: 10.1016/j.jhin.2017.06.023. Epub 2017 Jun 23. J Hosp Infect. 2017. PMID: 28651859
-
Central venous catheters and biofilms: where do we stand in 2017?APMIS. 2017 Apr;125(4):365-375. doi: 10.1111/apm.12665. APMIS. 2017. PMID: 28407421 Review.
Cited by
-
The Blood Microbiome and Health: Current Evidence, Controversies, and Challenges.Int J Mol Sci. 2023 Mar 15;24(6):5633. doi: 10.3390/ijms24065633. Int J Mol Sci. 2023. PMID: 36982702 Free PMC article. Review.
-
Does the antimicrobial-impregnated peripherally inserted central catheter decrease the CLABSI rate in neonates? Results from a retrospective cohort study.Front Pediatr. 2022 Nov 24;10:1012800. doi: 10.3389/fped.2022.1012800. eCollection 2022. Front Pediatr. 2022. PMID: 36507144 Free PMC article.
-
Neonatal intensive care unit (NICU) exposures exert a sustained influence on the progression of gut microbiota and metabolome in the first year of life.Sci Rep. 2021 Jan 14;11(1):1353. doi: 10.1038/s41598-020-80278-1. Sci Rep. 2021. PMID: 33446779 Free PMC article. Clinical Trial.
-
Assessment of the gut bacterial microbiome and metabolome of girls and women with Rett Syndrome.PLoS One. 2021 May 6;16(5):e0251231. doi: 10.1371/journal.pone.0251231. eCollection 2021. PLoS One. 2021. PMID: 33956889 Free PMC article.
-
Knowledge gaps in late-onset neonatal sepsis in preterm neonates: a roadmap for future research.Pediatr Res. 2022 Jan;91(2):368-379. doi: 10.1038/s41390-021-01721-1. Epub 2021 Sep 8. Pediatr Res. 2022. PMID: 34497356 Review.
References
-
- CDC. National HealthCare Safety Network Report. 2011.
-
- Payne NR, Carpenter JH, Badger GJ, Horbar JD, Rogowski J. Marginal increase in cost and excess length of stay associated with nosocomial bloodstream infections in surviving very low birth weight infants. Pediatrics. 2004;114(2):348–55. Epub 2004/08/03. doi: 114/2/348 [pii]. 10.1542/peds.114.2.348 . - DOI - PubMed
-
- Mahieu LM, De Dooy JJ, De Muynck AO, Van Melckebeke G, Ieven MM, Van Reempts PJ. Microbiology and risk factors for catheter exit-site and -hub colonization in neonatal intensive care unit patients. Infect Control Hosp Epidemiol. 2001;22(6):357–62. Epub 2001/08/25. doi: ICHE6828 [pii] 10.1086/501913 [doi]. . - DOI - PubMed
-
- Sitges-Serra A, Puig P, Linares J, Perez JL, Farrero N, Jaurrieta E, et al. Hub colonization as the initial step in an outbreak of catheter-related sepsis due to coagulase negative staphylococci during parenteral nutrition. JPEN J Parenter Enteral Nutr. 1984;8(6):668–72. Epub 1984/11/01. 10.1177/0148607184008006668 . - DOI - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
