

Maternal and birth cohort studies in the Gulf Cooperation Council countries: a systematic review and meta-analysis
- PMID: 31948468
- PMCID: PMC6964097
- DOI: 10.1186/s13643-020-1277-0
Maternal and birth cohort studies in the Gulf Cooperation Council countries: a systematic review and meta-analysis
Abstract
Background: We systematically reviewed and chronicled exposures and outcomes measured in the maternal and birth cohort studies in the Gulf Cooperation Council (GCC) countries and quantitatively summarized the weighted effect estimates between maternal obesity and (1) cesarean section (CS) and (2) fetal macrosomia.
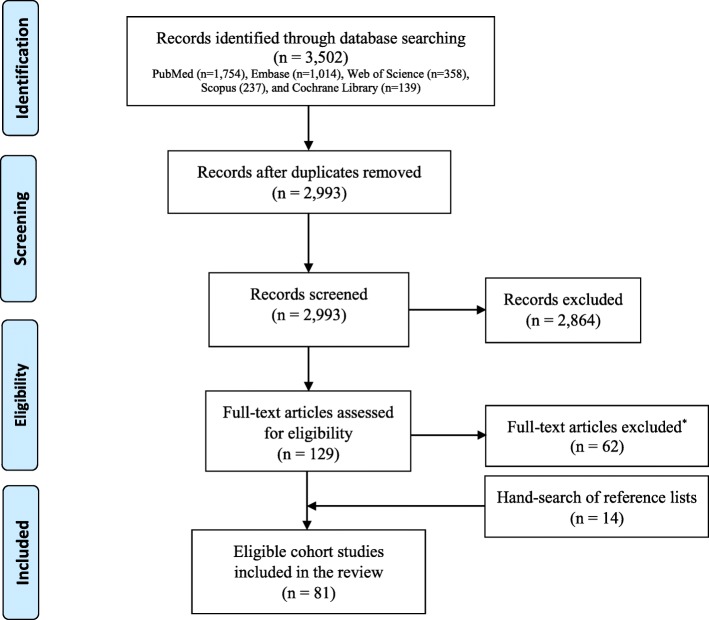
Methods: We searched MEDLINE-PubMed, Embase, Cochrane Library, Scopus, and Web of Science electronic databases up to 30 June 2019. We considered all maternal and birth cohort studies conducted in the six GCC countries (Bahrain, Kuwait, Oman, Qatar, Saudi Arabia, and United Arab Emirates (UAE)). We categorized cohort studies on the basis of the exposure(s) (anthropometric, environmental, medical, maternal/reproductive, perinatal, or socioeconomic) and outcome(s) (maternal or birth) being measured. Adjusted weighted effect estimates, in the form of relative risks, between maternal obesity and CS and fetal macrosomia were generated using a random-effects model.
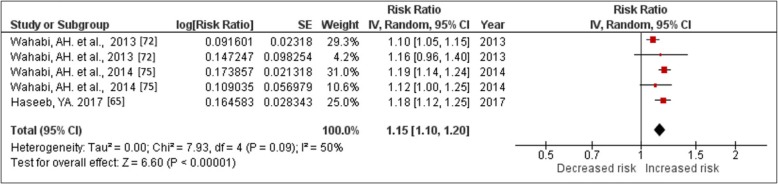
Results: Of 3502 citations, 81 published cohort studies were included. One cohort study was in Bahrain, eight in Kuwait, seven in Qatar, six in Oman, 52 in Saudi Arabia, and seven in the UAE. Majority of the exposures studied were maternal/reproductive (65.2%) or medical (39.5%). Birth and maternal outcomes were reported in 82.7% and in 74.1% of the cohort studies, respectively. In Saudi Arabia, babies born to obese women were at a higher risk of macrosomia (adjusted relative risk (aRR), 1.15; 95% confidence interval (CI), 1.10-1.20; I2 = 50%) or cesarean section (aRR, 1.21; 95% CI, 1.15-1.26; I2 = 62.0%). Several cohort studies were only descriptive without reporting the magnitude of the effect estimate between the assessed exposures and outcomes.
Conclusions: Cohort studies in the GCC have predominantly focused on reproductive and medical exposures. Obese pregnant women are at an increased risk of undergoing CS delivery or macrosomic births. Longer-term studies that explore a wider range of environmental and biological exposures and outcomes relevant to the GCC region are needed.
Systematic review registration: PROSPERO CRD42017068910.
Keywords: Cohort studies; Infant health; Maternal exposure; Maternal health; Middle East; Prenatal exposure delayed effects; Review.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Alberico S, Montico M, Barresi V, Monasta L, Businelli C, Soini V, et al. The role of gestational diabetes, pre-pregnancy body mass index and gestational weight gain on the risk of newborn macrosomia: results from a prospective multicentre study. BMC Pregnancy Childbirth. 2014;14:23. doi: 10.1186/1471-2393-14-23. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
