

Utilization and outcomes in biventricular assist device support in pediatrics
- PMID: 31948738
- PMCID: PMC7544019
- DOI: 10.1016/j.jtcvs.2019.11.068
Utilization and outcomes in biventricular assist device support in pediatrics
Abstract
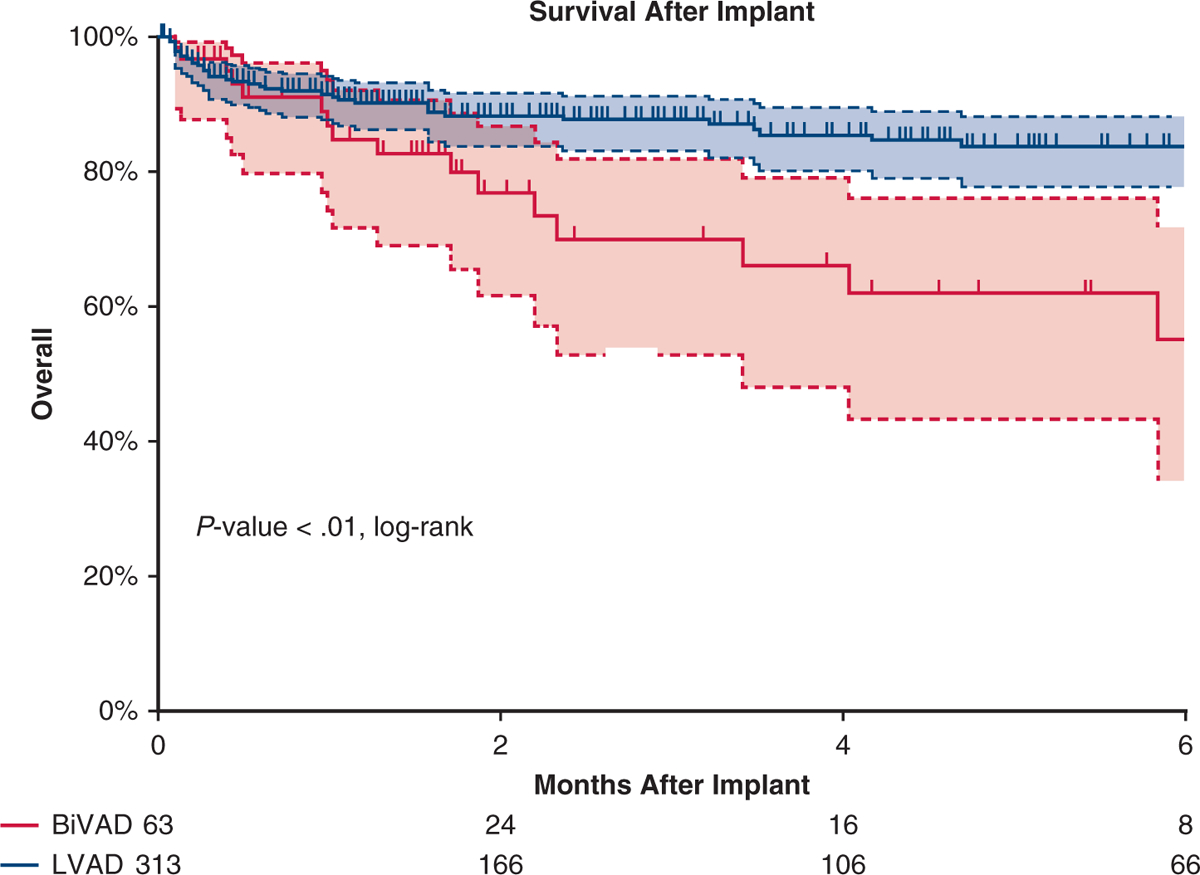
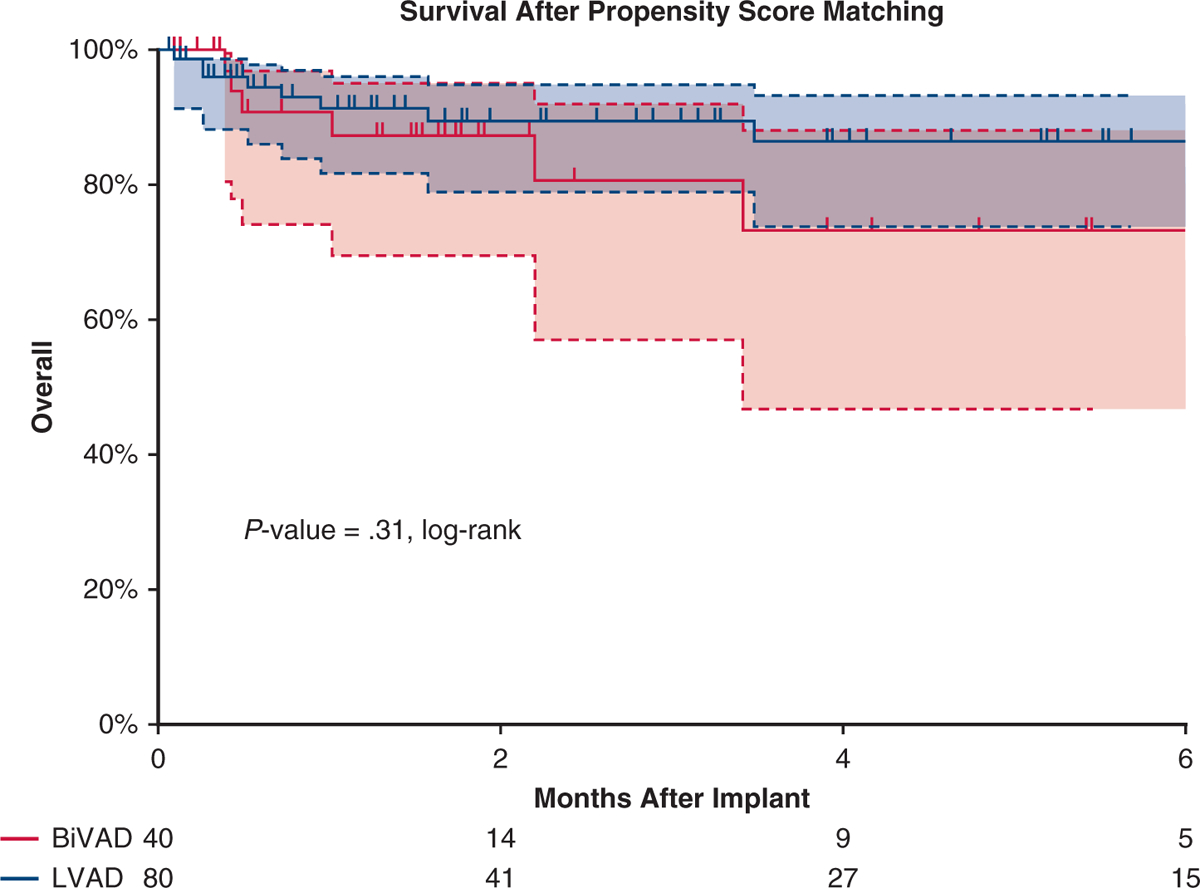
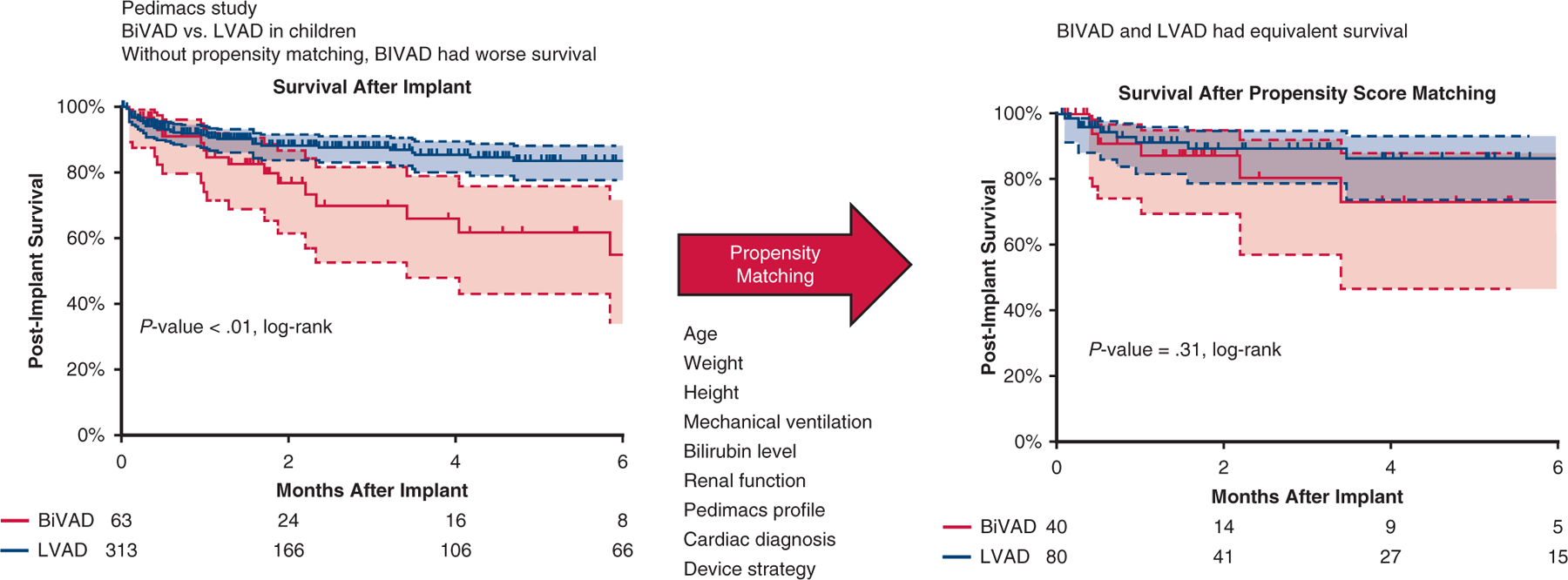
Objective: Patients with biventricular assist devices (BiVADs) have worse outcomes than those with left ventricular assist devices (LVADs). It is unclear whether these outcomes are due to device selection or patient factors. We used propensity score matching to reduce patient heterogeneity and compare outcomes in pediatric patients supported with BiVADs with a similar LVAD cohort.
Methods: The Pedimacs registry was queried for patients who were supported with BiVAD or LVAD. Patients were analyzed by BiVAD or LVAD at primary implant and the 2 groups were compared before and after using propensity score matching.
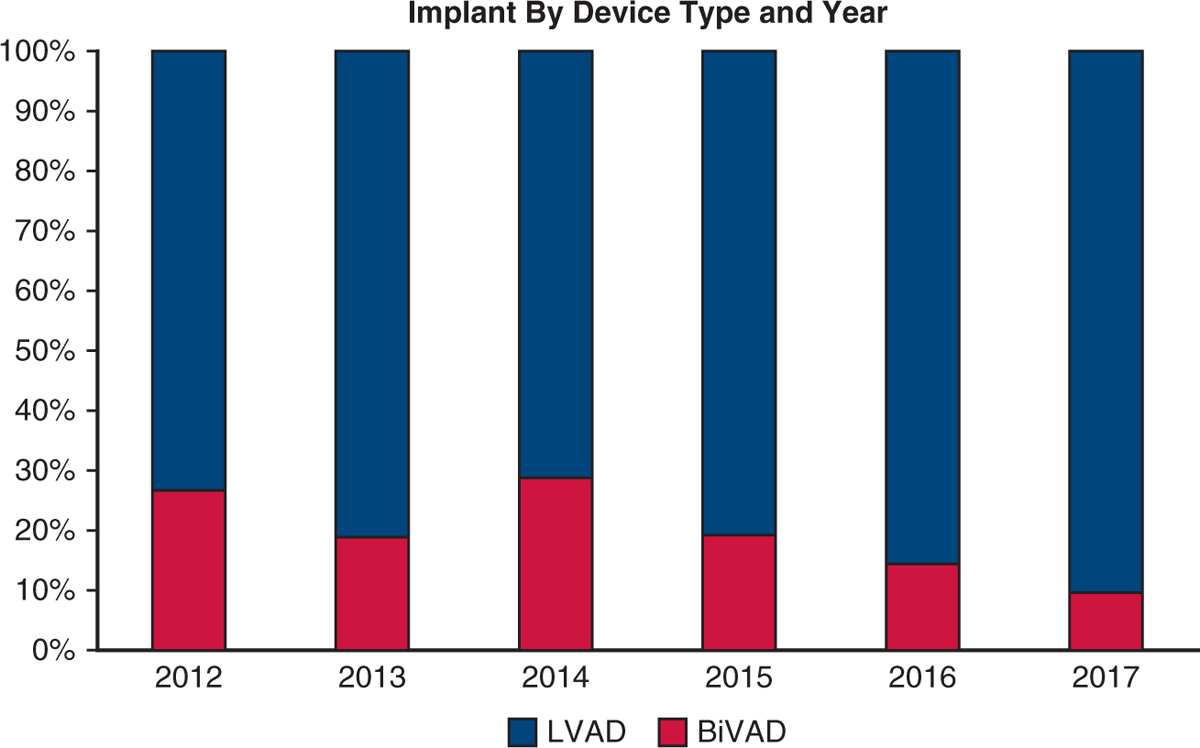
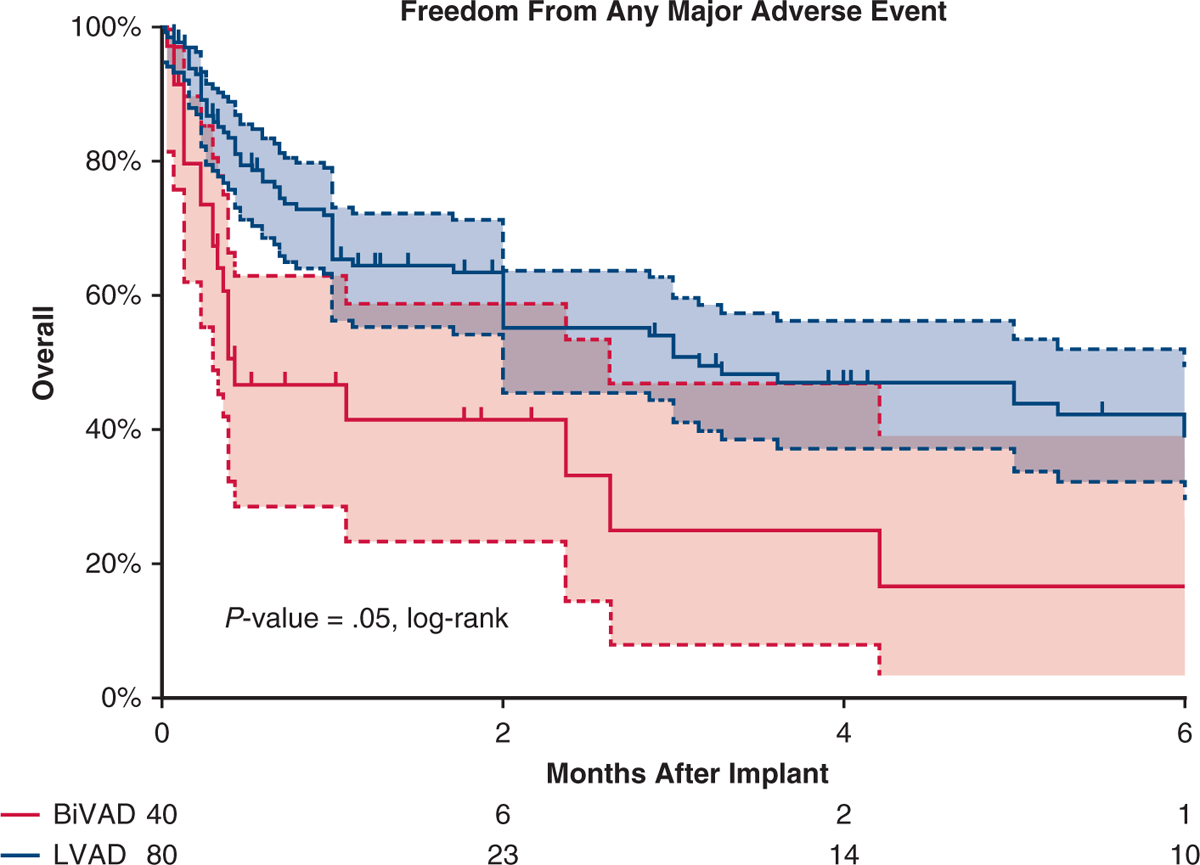
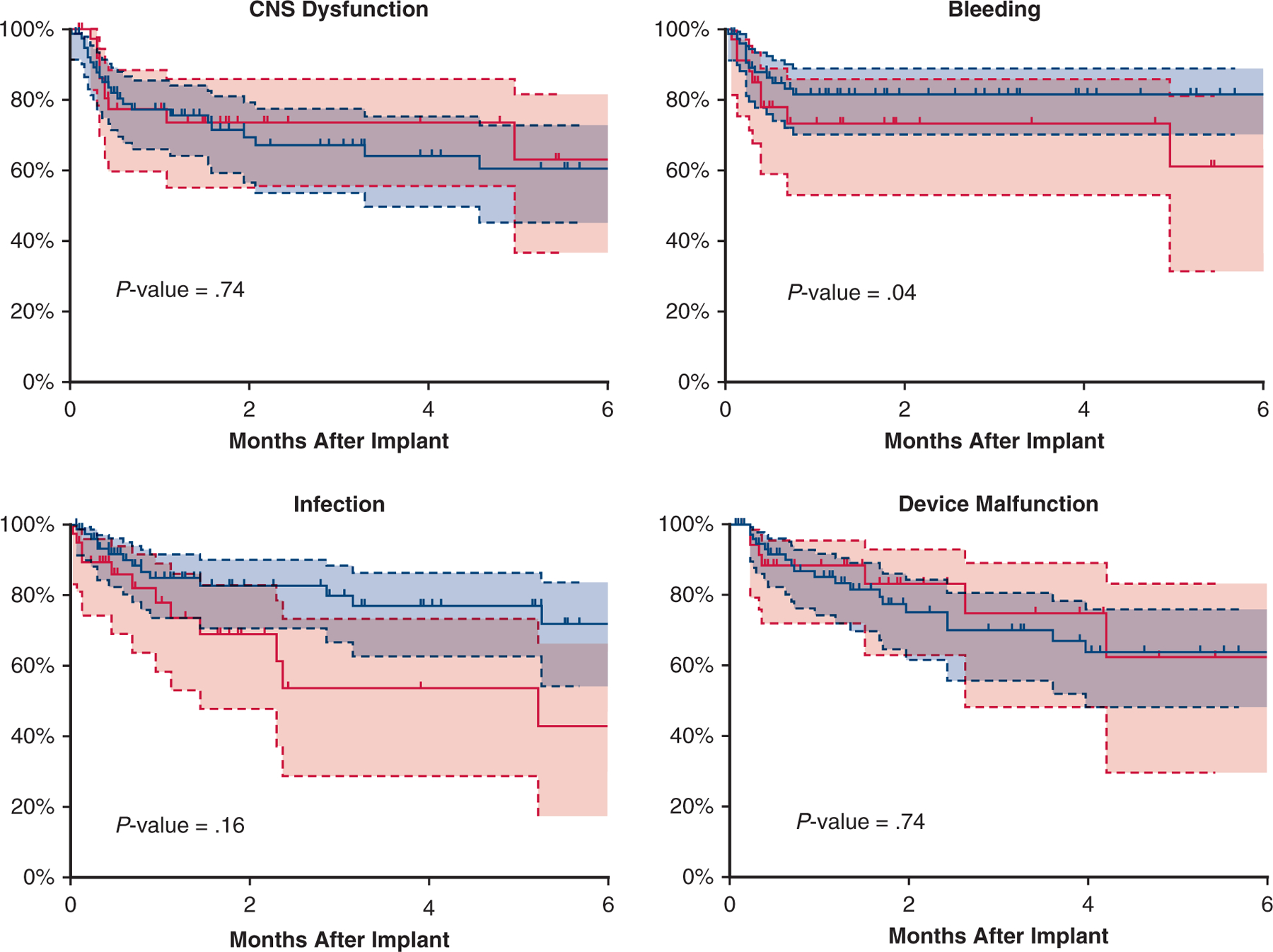
Results: Of 363 patients who met inclusion criteria, 63 (17%) underwent primary BiVAD support. After propensity score matching, differences between cohorts were reduced. Six months after implant, in the BiVAD cohort (LVAD cohort) 52.5% (42.5%) had been transplanted; 32.5% (40%) were alive with device, and 15% (10%) had died. Survival was similar between cohorts (P = .31, log-rank), but patients with BiVADs were more likely to experience a major adverse event in the form of bleeding (P = .04, log-rank). At 1 week and 1 and 3 months' postimplant, the percentage of patients on mechanical ventilation, on dialysis, or with elevated bilirubin was similar between the 2 groups.
Conclusions: When propensity scores were used to reduce differences in patient characteristics, there were no differences in survival but more major adverse events in the patients with BiVADs, particularly bleeding. Differences in unmatched patient outcomes between LVAD and BiVAD cohorts likely represent differences in severity of illness rather than mode of support.
Keywords: biventricular assist device; pediatrics.
Copyright © 2019 The American Association for Thoracic Surgery. Published by Elsevier Inc. All rights reserved.
Figures

Comment in
-
Commentary: To BiVAD or not to BiVAD…that is the question?J Thorac Cardiovasc Surg. 2020 Nov;160(5):1310-1311. doi: 10.1016/j.jtcvs.2020.01.003. Epub 2020 Jan 11. J Thorac Cardiovasc Surg. 2020. PMID: 32029209 No abstract available.
-
Commentary: Two sides of the same coin: Competing biventricular assist device outcomes from Pediatric Interagency Registry for Mechanical Circulatory Support data.J Thorac Cardiovasc Surg. 2020 Nov;160(5):1311-1312. doi: 10.1016/j.jtcvs.2019.12.078. Epub 2020 Jan 12. J Thorac Cardiovasc Surg. 2020. PMID: 32067790 No abstract available.
-
Commentary: Is two ever better than one in pediatric ventricular assist device support? The controversy continues.J Thorac Cardiovasc Surg. 2020 Nov;160(5):1309-1310. doi: 10.1016/j.jtcvs.2020.01.026. Epub 2020 Jan 31. J Thorac Cardiovasc Surg. 2020. PMID: 32107029 No abstract available.
References
-
- Peng E, Kirk R, Wrightson N, Duong P, Ferguson L, Griselli M, et al. An extended role of continuous flow device in pediatric mechanical circulatory support. Ann Thorac Surg. 2016;102:620–7. - PubMed
-
- Miera O, Kirk R, Buchholz H, Schmitt KR, VanderPluym C, Rebeyka IM, et al. A multicenter study of the HeartWare ventricular assist device in small children. J Heart Lung Transplant. 2016;35:679–81. - PubMed
-
- Deshpande SR, Carroll MM, Mao C, Mahle WT, Kanter K. Biventricular support with HeartWare ventricular assist device in a pediatric patient. Pediatr Transplant. 2018;22. - PubMed
-
- Almond CS, Morales DL, Blackstone EH, Turrentine MW, Imamura M, Massicotte MP, et al. Berlin Heart EXCOR pediatric ventricular assist device for bridge to heart transplantation in US children. Circulation. 2013;127: 1702–11. - PubMed
-
- Morales DL, Almond CS, Jaquiss RD, Rosenthal DN, Naftel DC, Massicotte MP, et al. Bridging children of all sizes to cardiac transplantation: the initial multicenter North American experience with the Berlin Heart EXCOR ventricular assist device. J Heart Lung Transplant. 2011;30:1–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
